Downloaded 1,859 times
![• Clearence:- volume of blood completely cleared
of a substance per unit of time.
• Renal Plasma Flow (RPF):- measured by p-
aminohippurate (PAH) clearance
RPF = clearence of PAH =
- [PAH]U = urinary concentration of PAH
- [PAH]P = plasma PAH concentration
• Renal Blood Flow (RBF)=
• Normally, RPF = 660mL/min and RBF = 1200mL/min](https://image.slidesharecdn.com/effectsofanesthesiaandsurgeryonrenalfunction-171218081721/85/Effects-of-anesthesia-and-surgery-on-renal-function-6-320.jpg)
![• Glomerular Filtration Rate (GFR):- Volume of fluid
filtered from the glomerular capillaries into
bowman’s capsule per unit time.
• Calculated using inulin or creatinine clearence.
[Creatinine]U:- creatinine concentration urine.
[Creatinine]P:- creatinine concentration plasma.
- Normal:- 120 ± 25 ml/min (male), 95 ± 20 ml/min (female)
• Filtration Fraction = GFR/RPF
- Normally:- 20%](https://image.slidesharecdn.com/effectsofanesthesiaandsurgeryonrenalfunction-171218081721/85/Effects-of-anesthesia-and-surgery-on-renal-function-7-320.jpg)
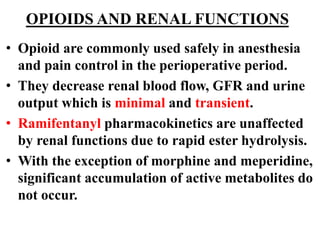
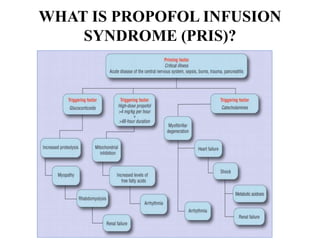
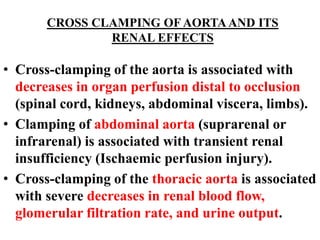

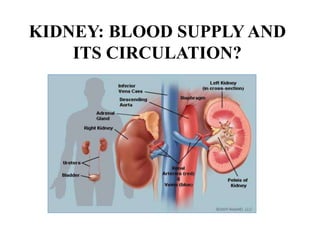
Anesthesia and surgery significantly affect renal function both directly and indirectly, primarily through hemodynamic changes. Inhalational anesthetics reduce glomerular filtration rate and urine output, while opioids and intravenous agents can also impact renal function, with varying effects based on their usage and the patient's condition. Notable factors affecting renal performance during anesthesia include hydration, positioning, surgical stress, and mechanical ventilation.

































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

