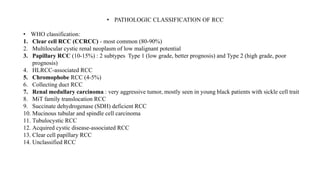
Renal cell carcinoma (RCC) is the most common kidney cancer, especially in adults aged 50-70, and is mostly of clear cell histology. Risk factors include smoking, obesity, and hypertension, while hereditary syndromes can present atypically. Treatment strategies vary by cancer stage, primarily involving surgery and increasing use of systemic therapies like targeted immunotherapy.







































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






