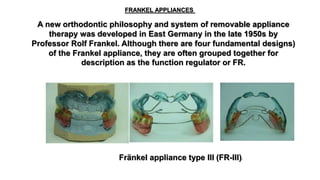
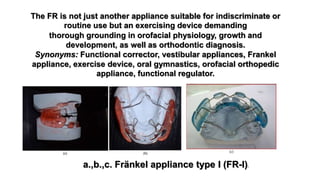
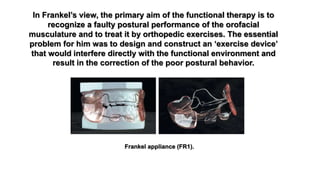
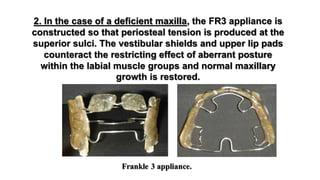
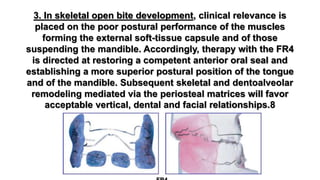
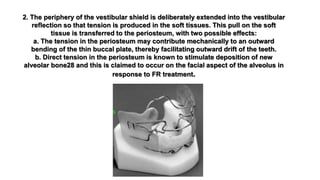
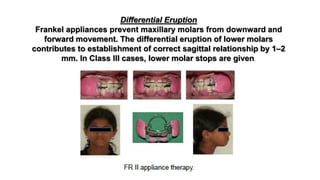
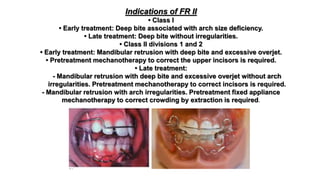
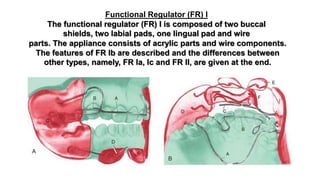
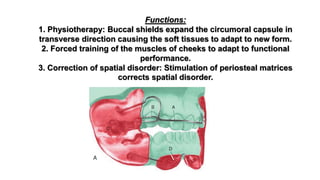
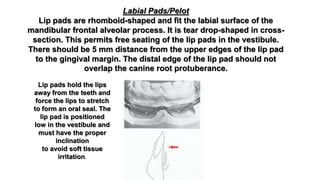
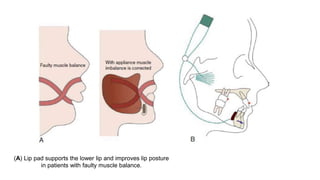
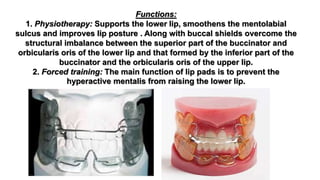
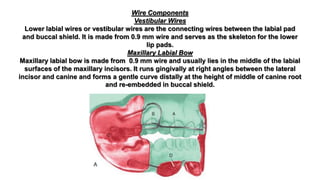
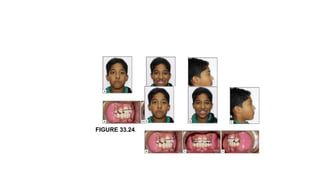
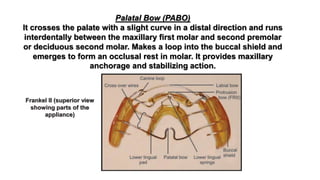
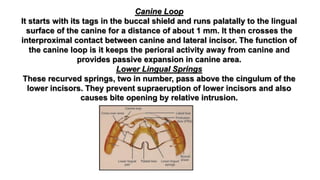
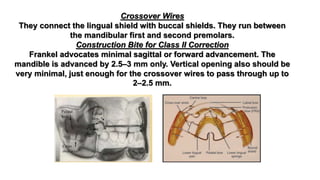
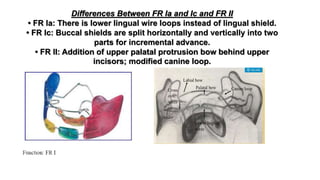
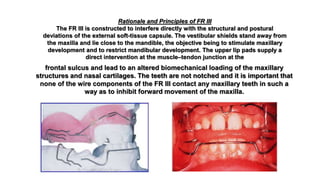
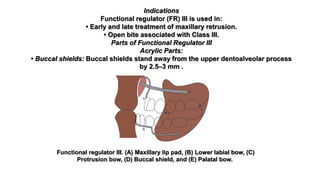
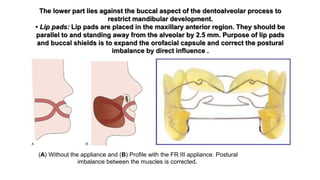
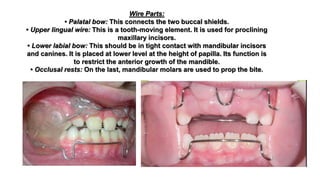
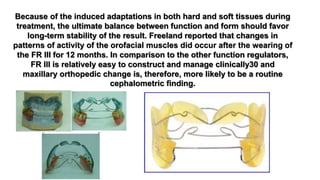
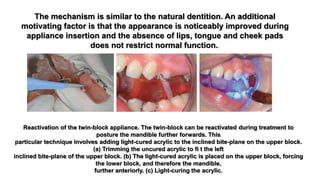
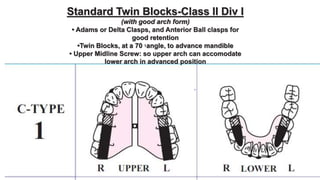
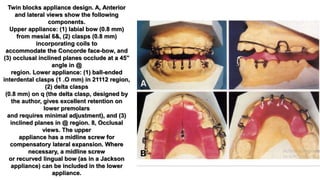
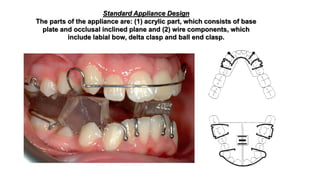
This document describes the Frankel appliance, a type of removable functional orthodontic appliance developed in the 1950s. It summarizes the four main types of Frankel appliances (FR I-IV) and their indications. The key components and mechanisms of action of the FR I appliance are described in detail, including its acrylic parts (buccal shields, labial pads, lingual shield) and how they work to correct muscle posture and spatial disorders through forces on the periosteum.