Downloaded 261 times

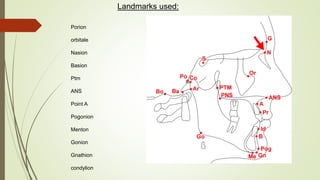
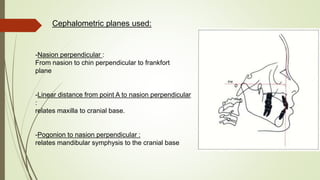




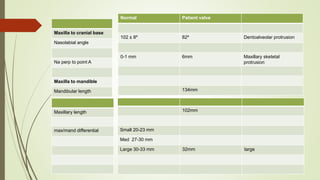
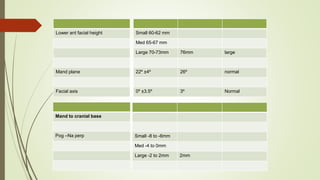
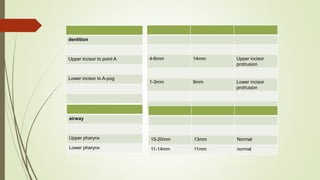

Dr. James McNamara developed a cephalometric analysis method in 1984 to evaluate orthodontic and orthognathic surgery patients. The analysis divides the craniofacial skeleton into five sections - maxilla to cranial base, maxilla to mandible, mandible to cranial base, dentition, and airway. Linear measurements of landmarks and planes are compared to normative standards to assess relationships. Advantages include using primarily linear measurements, being more sensitive to vertical changes, and providing growth guidelines that are easily explained.



































































