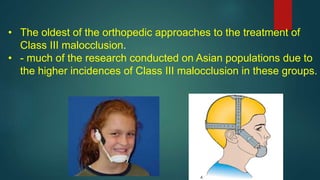
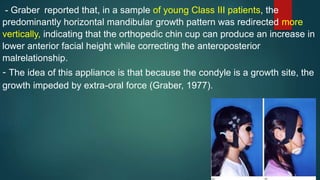
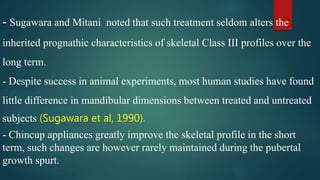
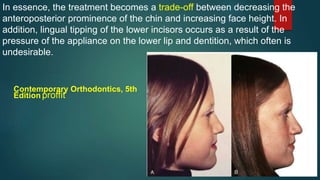
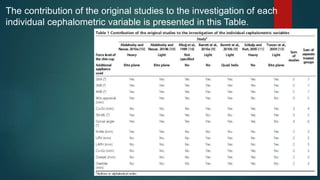
Chin cups are a traditional orthopedic appliance used to treat Class III malocclusions. While some studies have found chin cups can temporarily retard mandibular growth and correct the malocclusion through backward rotation, the effects are not consistently maintained long-term. Meta-analyses found chin cups significantly reduced SNB angle and increased ANB and Wits appraisal in the short-term, but heterogeneity between studies was high. Chin cups also increased SN-ML angle and decreased gonial angle, indicating a tendency for increased vertical growth and posterior mandibular rotation. However, long-term stability and the effects of vertical chin cups require more research due to limited data.







































![FACEMASK CHINCUP SEMINAR[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/facemaskchincupseminar1-230916061625-e0964de8-thumbnail.jpg?width=640&height=640&fit=bounds)