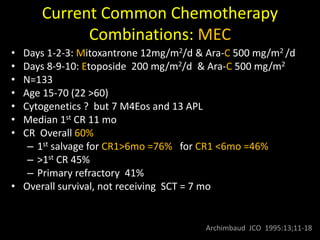
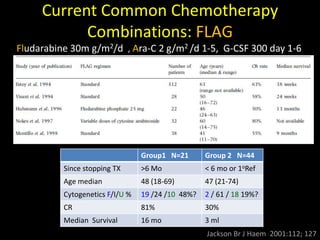
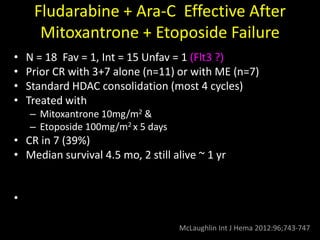
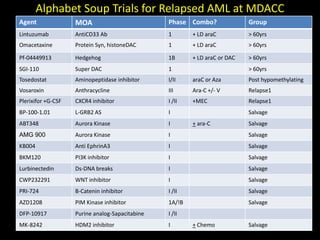
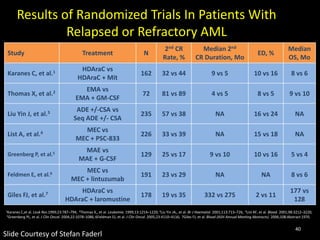
1) Current chemotherapy combinations for relapsed AML such as MEC (mitoxantrone, etoposide, cytarabine) and FLAG (fludarabine, cytarabine, G-CSF) produce overall response rates of 40-60% but have not been shown to be clearly superior to one another.
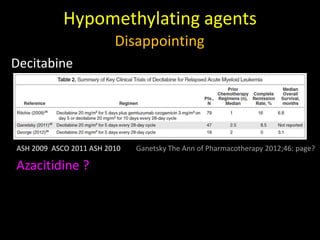
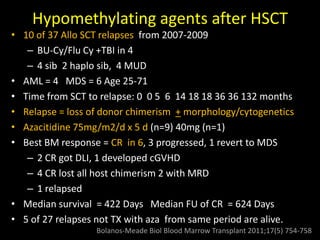
2) Single agent therapies approved for relapsed AML include hypomethylating agents, immunomodulatory drugs, and targeted therapies but have shown limited and disappointing efficacy as single agents.
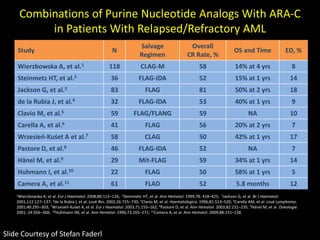
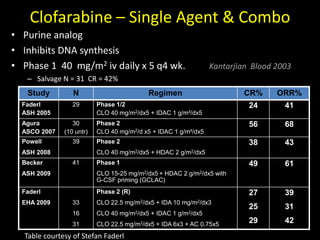
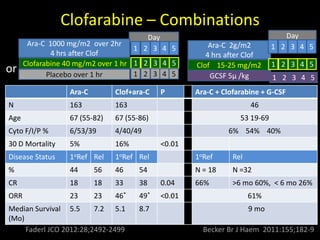
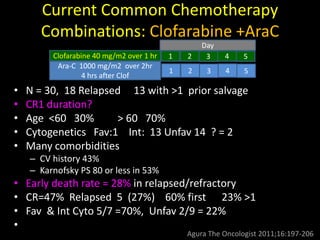
3) Clofarabine has shown efficacy in combinations with cytarabine for relapsed AML, with complete response rates as high as 50% in some studies