Downloaded 66 times







































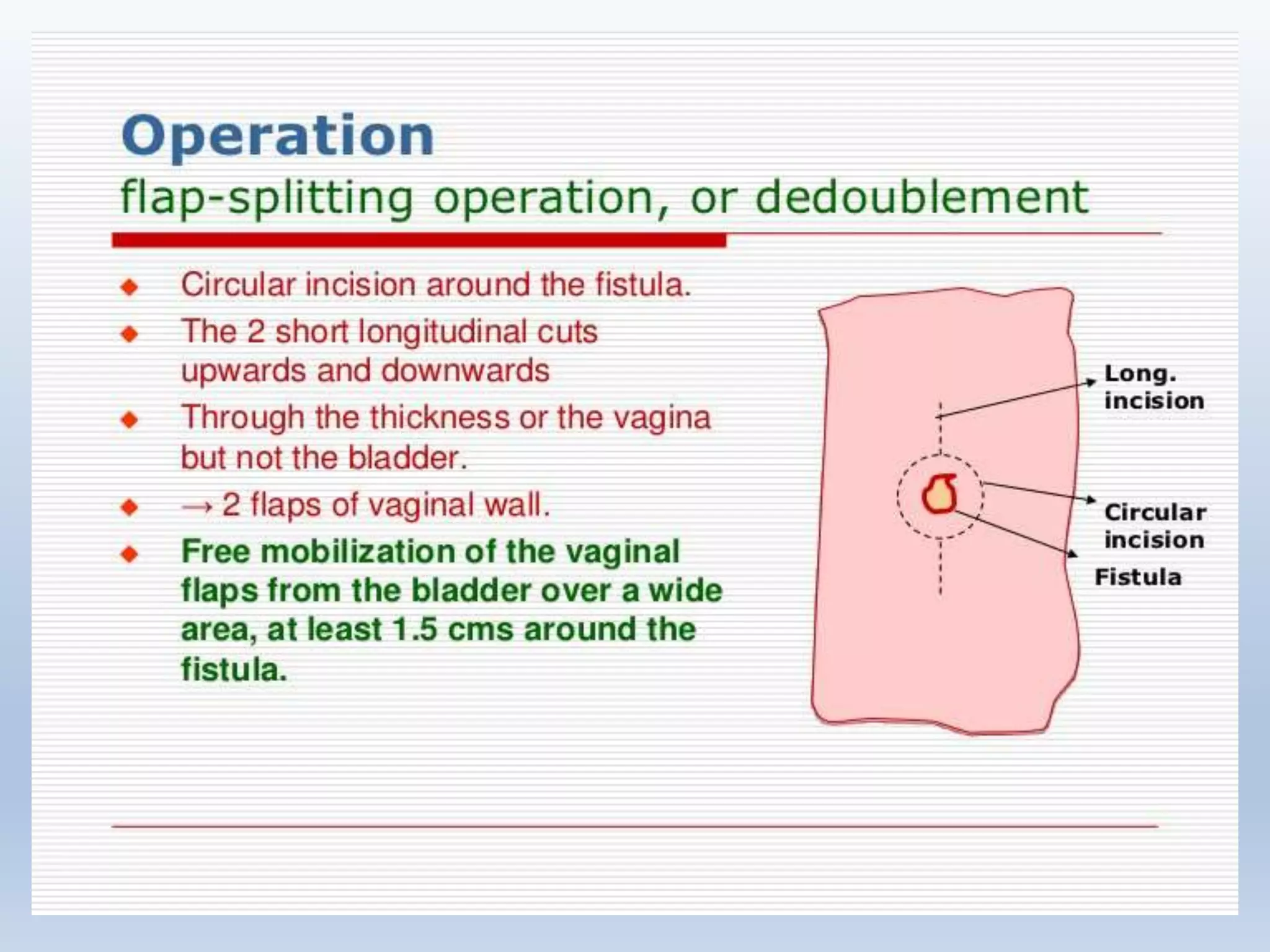
































An obstetric fistula is an abnormal connection between the vagina and bladder or rectum, usually caused by prolonged labor without prompt medical care. Symptoms include constant urinary or fecal incontinence. Management involves initial catheterization followed by surgical repair once tissues have healed, usually 3 months later. Surgical techniques depend on the location and complexity of the fistula. Post-operative care focuses on drainage and preventing infection to allow healing.























































































