Downloaded 153 times



![Remodeling Phase
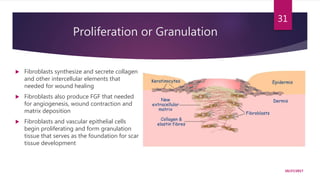
The principle cell involved in this process is the fibroblast. When the levels of
collagen production and degradation equalize, the maturation phase of tissue
repair is said to have begun] During maturation, type III collagen, which is
prevalent during proliferation, is replaced by type I collagen. Originally
disorganized collagen fibers are rearranged, cross-linked, and aligned along
tension lines.
Remodeling can take up to 2 years after wounding.
10/27/2017
32](https://image.slidesharecdn.com/woundhealing-171027114458/85/Wound-healing-32-320.jpg)







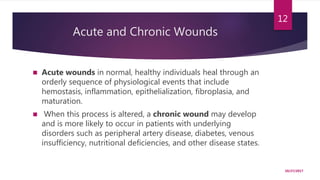
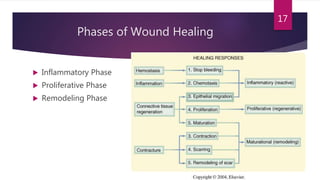
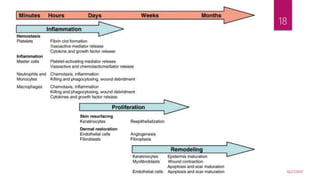
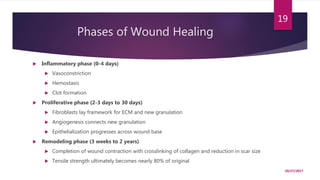
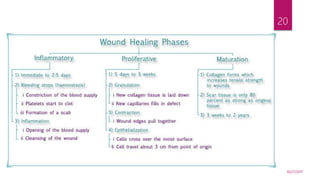
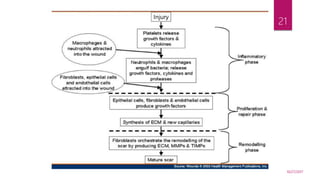
This document provides an overview of wound healing, including definitions of wounds, the wound healing process, and chronic wounds. It discusses the three main phases of wound healing: inflammatory, proliferative, and remodeling. Key points include that acute wounds normally heal in an orderly process, while chronic wounds fail to progress and are associated with underlying conditions. The document also covers wound classification, growth factors involved in healing, cell types proliferating during each phase, and factors that can impair the wound healing process.



















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















