Downloaded 70 times


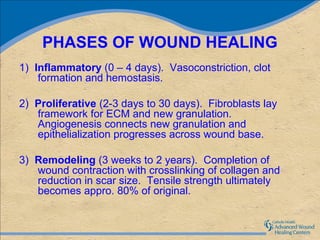
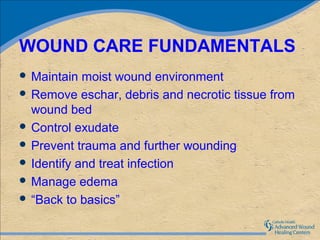
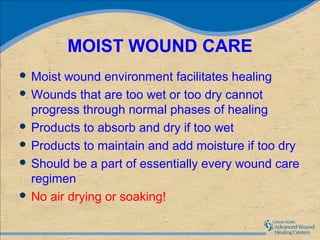













1) The document discusses various wound care products and their uses. It describes phases of wound healing and fundamentals of wound care. 2) It provides details on different dressing types including hydrocolloids, calcium alginates, hydrogels, foams, silver products, collagen dressings, film dressings, and bioengineered skin substitutes. 3) The document advises that the appropriate product depends on factors like the wound's needs to promote healing, practical considerations, and the patient's situation.












































































