Downloaded 37 times

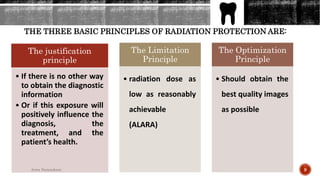








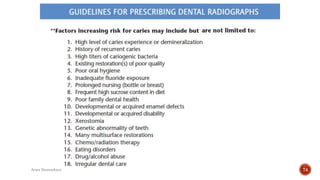


The document discusses key aspects of radiology, highlighting its role in diagnosis and treatment planning, particularly in identifying dental conditions. It covers radiation safety principles, various radiographic techniques and image receptors, and guidelines for appropriate radiographic examinations tailored to patient needs. Additionally, it emphasizes the importance of professional judgment in utilizing radiography, especially for special-needs patients.



































































