The document discusses splenomegaly (enlarged spleen). It provides information on:
- The spleen's functions including filtering blood and housing immune cells.
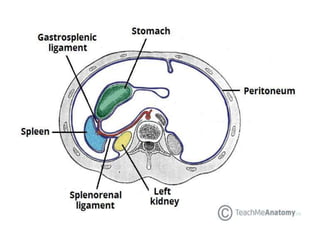
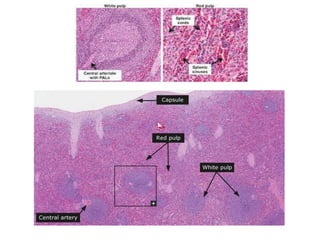
- Anatomical details such as blood flow patterns and composition of red and white pulp.
- Normal spleen size and location within the rib cage.
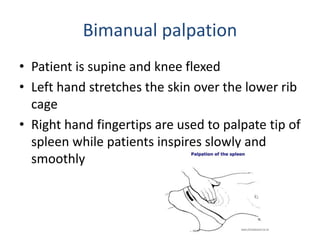
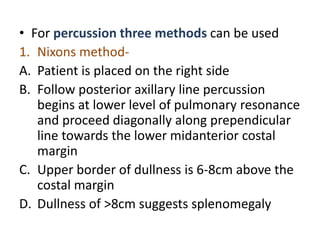
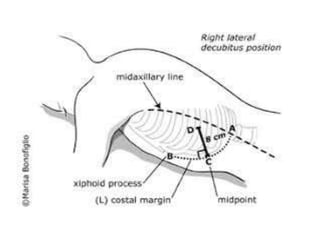
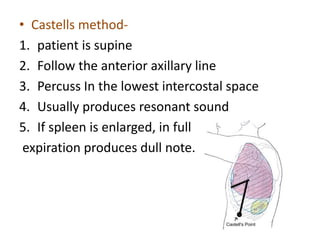
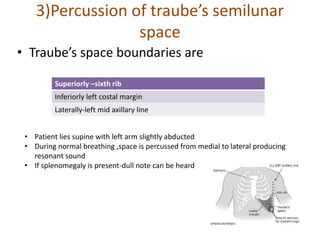
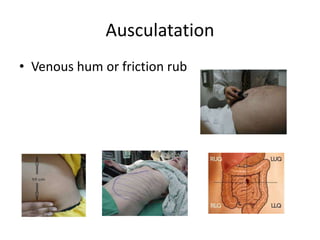
- Physical examination techniques for evaluating spleen size such as percussion and palpation.
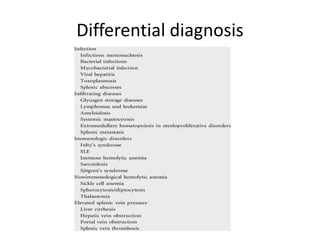
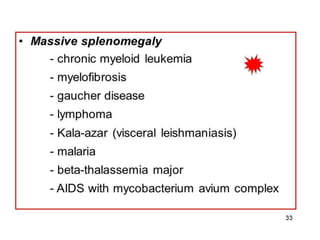
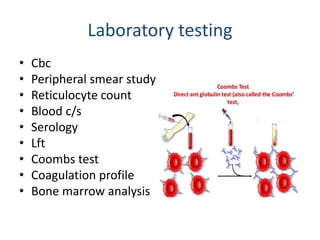
- Causes of splenomegaly and complications like pain or rupture. Management includes treating underlying causes and possible splenectomy for severe cases.


































![[Int. med] spleenomegaly from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/vcnwsy2ltcejz2qexiuf-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171704-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)

































