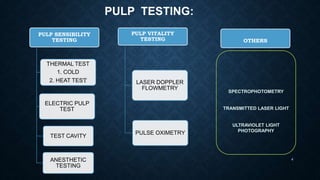
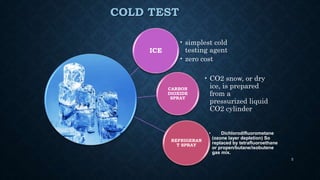
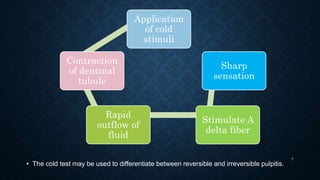
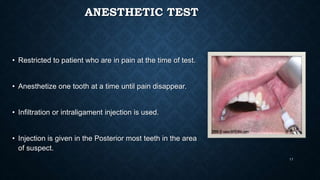
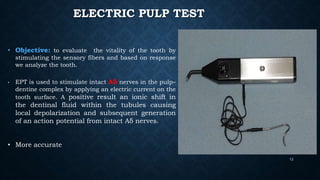
This document discusses various methods for assessing pulp vitality, including thermal tests using cold or heat, electric pulp testing, anesthetic testing, test cavity preparation, laser Doppler flowmetry, and pulse oximetry. Thermal tests involve applying cold or hot stimuli to elicit responses from Aδ or C nerve fibers to determine if the pulp is reversible or irreversibly inflamed. Electric pulp testing uses electricity to stimulate Aδ nerves and assess response. Laser Doppler flowmetry and pulse oximetry are non-invasive methods that use lasers or light to measure blood flow and oxygen saturation to determine pulp vitality. Each method has advantages and limitations for accurately assessing the status of the dental pulp.