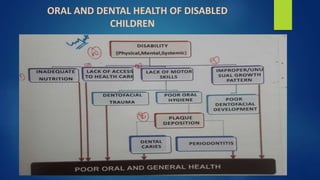
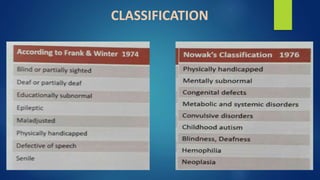
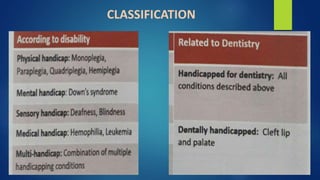
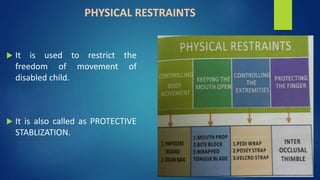
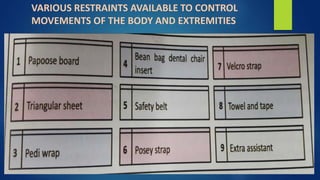
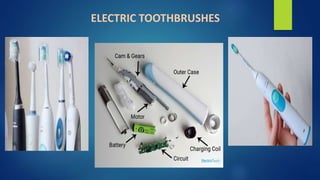
The document discusses the assessment, diagnosis, and treatment of dental issues in handicapped children. It defines a handicapped child as someone who cannot achieve their full potential compared to others due to mental, physical, medical, or social conditions. An initial dental exam is important to establish care and a good relationship with parents. Radiographs can aid diagnosis. The goals of treatment are efficient care with minimal trauma. Restraints may be needed to control movements. Establishing a "dental home" improves preventive care and reduces costs. Home dental care from infancy is advised. Electric toothbrushes and fluoride can aid plaque control. Mentally challenged children often have dental neglect and caries, so maintenance of oral hygiene