Vitality Test:
• Theseare used to determine the vitality or non vitality of the
dental pulp
• Vitality test may also provide a rough guide to states of
inflammatory change of the pulp
• Vitality test results do not correlate well with the histological
changes occurring within the pulp.
• Testing should begin on a normal, healthy tooth, rather than a
painful tooth likely to provide an exaggerated response, to
allow the patients fear.
• Testing stimuli should be applied to normal enamel of the
crown of the tooth, avoiding any restorations and soft tissues;
10.
The Following vitalitytests are described
Thermal
Electrical
Diagnostic access cavity, without
anesthesia.
• A healthytooth with a vital, non inflamed pulp
can usually be stimulated within a
temperature range of some 20-50 C without
pain.
• Teeth with inflamed pulps (Pulpitis) may react
with severe pain on temperature stimulation
even within the above range.
18.
Cold:
A pledged ofcotton wool, held in college
tweezers, is soaked in Ethyl chloride. As the
ethyl chloride evaporates, ice crystals form on
the pledged. The ice pledged is then applied to
the tooth.
19.
Heat:
A gutta perchastick is heated in a flame until
the tip softens. The hot tip is then applied to
the tooth. If the tooth is previously lightly
vaslined, the softens gutta percha will not
adhere to the tooth.
Electrical Vitality Test:
•These offer the advantage of a more controlled, graded
stimulus in comparison with thermal test, as most
machines offer a digital display of the stimulus level.
• The tooth to be tested must be isolated with cotton wool
rolls and dried. Any moisture on the tooth may conduct
electricity into the soft tissues. The electrode in contact
with a tooth should not be placed on a restoration, plastic
restoratives are electrical insulators, while metals may
conduct electricity to the gingival tissues or an adjacent
tooth. The electrode must not contact soft tissues.
– The voltage should be gradually increased until a response is
elicited.
Positive (Normal)
• Thetest tooth responds in a similar way and to a similar
level of stimulation to the other healthy teeth.
• This results suggest that the pulp is vital and not inflamed.
28.
Exaggerated , Brief:
•The test tooth responds more severely than other healthy
teeth and/or to a lower level of stimulation.
• The painful response last for less than some 15 seconds
after removal of the stimulus.
• The tooth may respond more to cold than heat stimulation.
Results
• This results suggest that the pulp is vital but inflamed;
Hyperaemia
• The pulpitis may be reversible if the cause is eliminated.
• Alternatively, Dentin may simply be exposed as a result of a
Crack, Caries, Leaking restoration or exposed and sensitive
root dentine.
29.
Exaggerated, Prolonged:
The testtooth responds more severely than other healthy teeth
and/or to a lower level of stimulation.
The painful response lasts for more than 15 seconds and
occasionally minutes or even hours, after removal of the stimulus.
The response to heat and electrical stimulation may be greater
than to cold. Indeed cold may reduce the pain.
Results:
This results suggest that the pulp is vital but inflamed, eg. acute pulpitis.
The pulpitis is likely to be Irreversible .
Note: A very gradual reaction to heat but not to cold or electric
stimulation, leading ultimately to an exaggerated response, may
indicate Chronic pulpitis.
30.
Negative:
• The testtooth does not respond to stimulation
but healthy tooth do.
Results:
This results suggest that the pulp is non-vital and
may be necrotic, or that the root canals are
sclerosed.
31.
False Positive:
•The testteeth responds normally but subsequent
events prove the Pulpal condition to be abnormal.
Results:
In Multi Rooted Teeth: Vital tissue remains in one root
but the remaining pulp is necrotic.
•In a Root Canal Filled with Pus: conducts stimuli.
•In a Root Canal Filled with Gas: Heat causes expansion.
•A frightened pt or a patient with a low pain
threshold may report a painful response even before
the stimulus is applied to the tooth.
32.
False Negative:
• Thetest tooth does not respond to stimulation
but subsequent events prove the pulp to be vital.
Result:
• If the pulp is well insulated from thermal and
electrical stimuli eg. Plastic restoration, secondary
dentine
• If the nerve supply to the pulp is damaged, eg:
Trauma.
• In patient with a high pain threshold
With faulty technique or equipment
33.
Inconclusive:
• All teethgive exaggerated responses or, conversely,
no teeth respond!
• If the results of two tests (e.g. Heat and cold) are
inconclusive, add a third test (e.g. electric ). If
doubt still exists, consider cutting a diagnostic
access cavity, without local anesthesia.
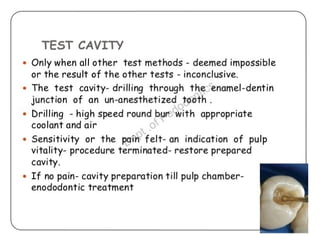
Diagnostic Access Cavitywithout Local Anesthesia:
• Cutting a small cavity in the suspect tooth without
anesthesia is probably the most reliable vitality test.
• If the pulp is vital, a response is usually elicited as
the dentine is entered.
• Since this test is destructive, it should be
considered only as a last resort.
46.
Percussion Tests:
•These areconducted by gently tapping a tooth with the tip of a dental
mirror handle.
•Two characteristics are noted:
Tenderness to percussion
A dull percussion note
•Both characteristics denote inflammation of the periodontal ligament.
•Greater tenderness to percussion in an apical direction suggest apical
periodontitis.
•Greater tenderness to percussion in a lateral direction suggests acute
periodontitis of gingival origin (Lateral Periodontitis).
•Testing should begin on a healthy tooth.
•Percussion testing must be conducted with great care since teeth with
periodontitis may be exquisitely tender.
47.
Mobility:
• Tooth mobilityis assessed by use of two instrument handles
---one placed buccal and the other lingual on the tooth.
• Alternatively a finger may substitute for one of the
instruments.
48.
Increased Mobility iscaused by:
• Reduced Bone Support:
Periodontal disease
Bony cyst
Neoplasm
• Abscess or inflammation of the periodontal ligament:
Acute periodontitis
Periodontitis of gingival origin
Occlusal trauma
Acute trauma
• Crown or Root fracture
• Fracture of supporting bone.
49.
Transillumination Test:
• Adedicated light source is needed.
• Alternatively, A composite curing light may be
employed.
Transillumination is useful in the diagnosis of:
• Tooth cracks
• Interproximal caries in anterior teeth
• Interproximal caries in posterior teeth, where
there is sufficient access.
58.
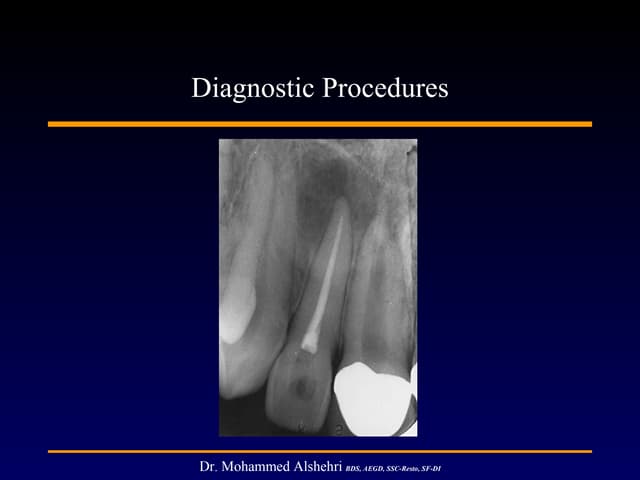
Radiography:
• Indication ofBitewing X-Ray:
- Crowns of teeth
- Caries, particularly interproximal lesions
- restorations
- Alveolar bone height
- Extension of fissure caries into dentine (if the
lesion is large)
• Periapical:
- Root and surrounding bone
59.
Radiography:
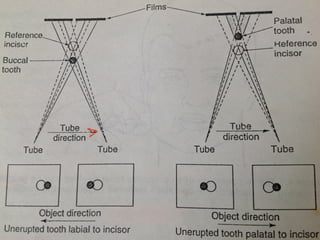
• Parallax Technique:
-Two periapical films, exposed at slightly
different anteroposterior angulation for the
assesment of buccolingual position of unerupted
tooth, particularly maxillary canines.
- The most Palatal tooth appears to move in the
same direction as the tube is is moved.
- The most Buccal tooth appears to move in the
opposite direction to the tube.
61.
Radiography:
• Pan Oral/Orthopantomogram/OPG
- General view of teeth, Jaws, Temporomandibular
joints, maxillary sinuses etc. Detail in the midline is
obscured by superimposition of the cervical spine.
– Lateral Oblique: General view, as OPG. May be used
where panoral/OPG facilities are not available.
– Maxillary Anterior Occlusal: Roots of maxillary
anterior teeth
– Mandibular Occlusal: Calcification in the floor of the
mouth, including submandibular gland and duct,
Buccolingual displacement of mandibular fractures.
62.
Radiography:
• Transpharyngeal: Temporomandibularjoint
• Occipitomental View (OMV) / PNS: Maxillary
sinuses, Facial & skull bones.
• Postero-anterior and lateral skull: Skull and
facial bones. Useful in Orthodontic assesment.