Downloaded 75 times

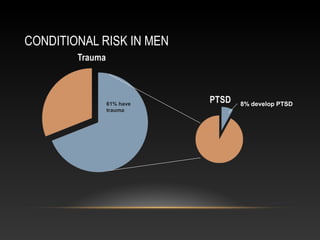
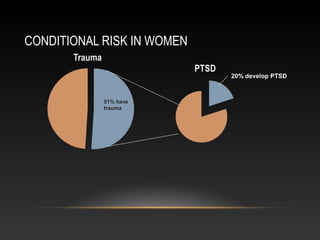
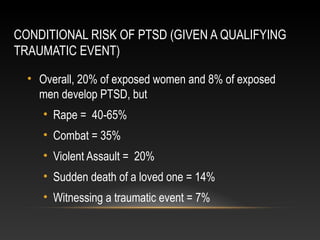
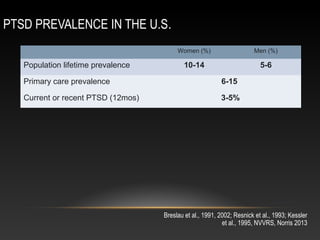
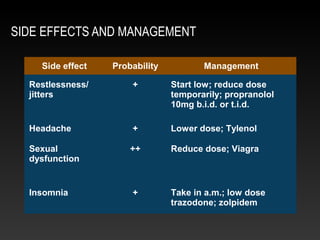

This document summarizes a presentation on posttraumatic stress disorder (PTSD) given by Dr. David Eisenman. Some key points: - Around 55% of US adults experience a traumatic event in their lifetime, but only 8-20% of those exposed develop PTSD depending on gender and type of trauma. - PTSD is characterized by intrusive memories, avoidance, negative alterations in mood/cognition, and hyperarousal. The DSM-5 made some changes to these criteria. - PTSD commonly co-occurs with depression, substance abuse, and physical symptoms. It is important to assess for these comorbidities. - First-line treatment involves SSRIs or SNRIs. Psych

















































![Original aapb alba presentation 2-97-2003-march [autosaved] (2 - copy](https://cdn.slidesharecdn.com/ss_thumbnails/originalaapbalbapresentation-2-97-2003-marchautosaved2-copy-160721070506-thumbnail.jpg?width=640&height=640&fit=bounds)













































