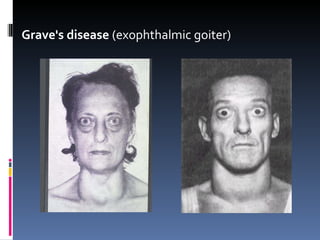
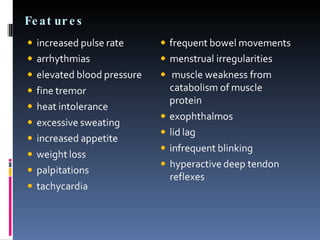
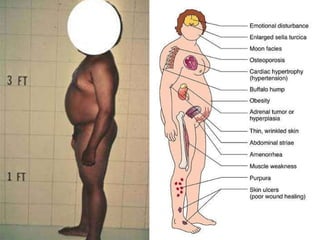
The document discusses several endocrine disorders and their psychiatric manifestations. Hyperthyroidism can cause nervousness, fatigue, insomnia, mood lability and other symptoms. Graves' disease is treated with antithyroid drugs, radioactive iodine or surgery. Hypothyroidism can cause depression, lethargy and cognitive impairments and is treated with thyroid hormone replacement. Cushing's syndrome due to hypercortisolism can result in mood changes like depression as well as physical signs. Hyperprolactinemia is associated with depression, stress intolerance and irritability. Certain disorders of the pituitary and adrenal glands can also impact mood and cognition.





![Treatment and Course Treatment of pituitary ACTH-producing tumors surgical resection pituitary irradiation Adrenal adenomas and carcinomas removed surgically chemotherapy is instituted in case of carcinoma Medications that antagonize cortisol production metyrapone or mitotane [tysobren] Medications that suppress ACTH serotonin antagonists (eg. cyproheptadine [Periactin]) Prednisone treatment, lithium and neuroleptic medications help prevent the development of manic or psychotic symptoms](https://image.slidesharecdn.com/psychosis2-100301095216-phpapp01/85/Psychosis2-26-320.jpg)
![Treatment Acute adrenal insufficiency requires immediate treatment with intravenous hydrocortisone in addition to fluid replacement with saline solution and potassium supplementation Primary adrenal insufficiency Mineralocorticoid e.g., fludrocortisone [Florinef] Chronic adrenal insufficiency prednisone or hydrocortisone is administered orally as maintenance treat](https://image.slidesharecdn.com/psychosis2-100301095216-phpapp01/85/Psychosis2-30-320.jpg)























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


