Downloaded 44 times


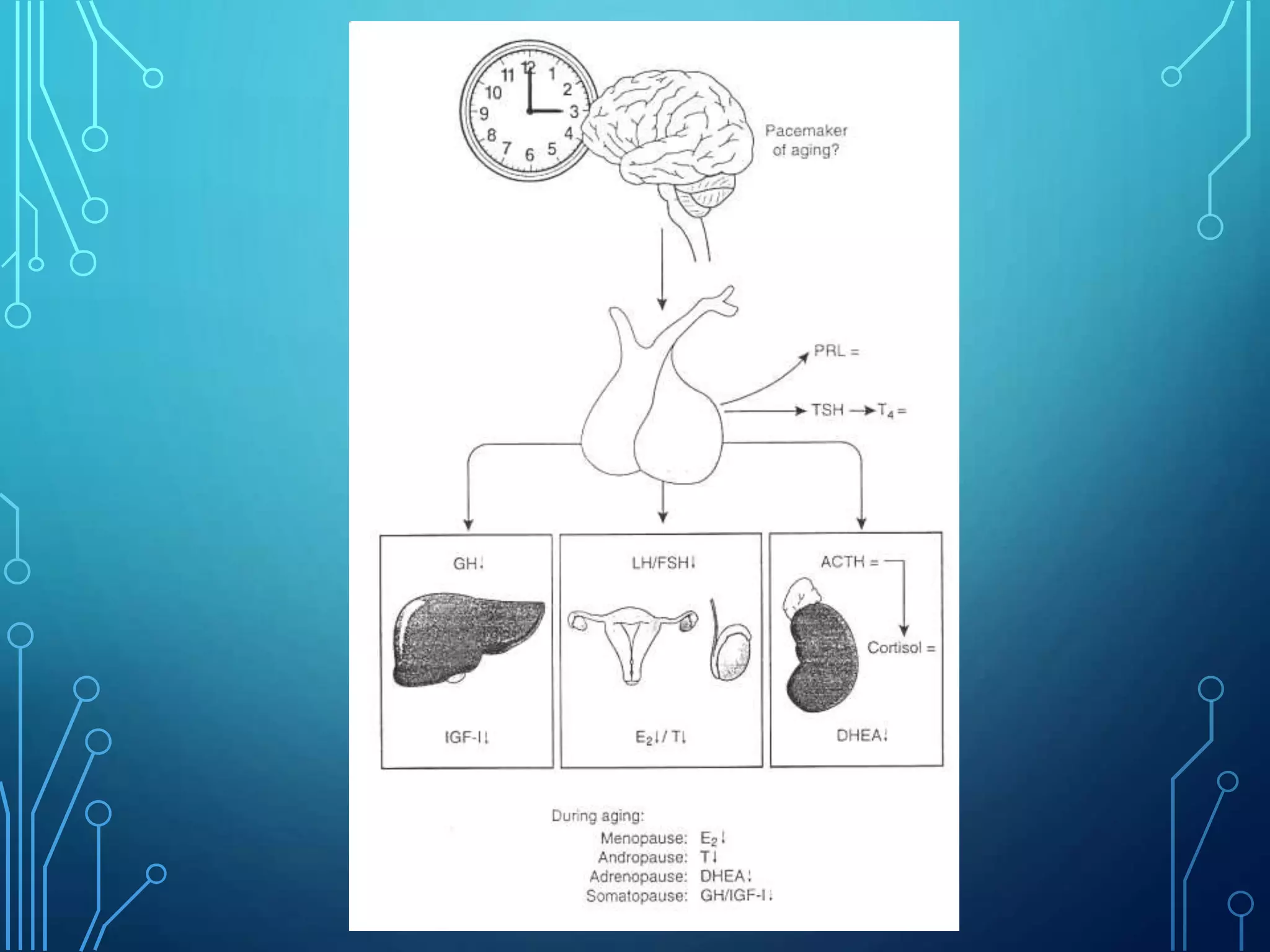













The document discusses age-related changes to the endocrine system. It covers changes to the hypothalamic-pituitary-adrenal axis, growth hormone, thyroid, adrenal cortex and medulla, pancreas, and hypothalamic-pituitary-testicular axis. Key effects of aging include decreased hormone production and feedback inhibition as well as increased pituitary and adrenal involvement in stress response. Diagnosing endocrine disorders can also be challenging in elderly patients due to nonspecific symptoms and normal age-related endocrine changes.











































![endo [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/endoautosaved-230213074450-6409a089-thumbnail.jpg?width=640&height=640&fit=bounds)























