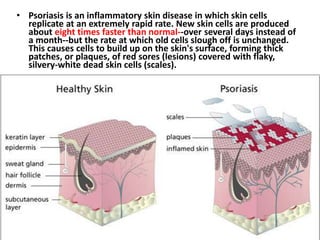
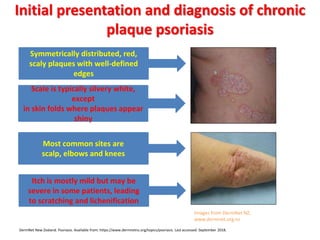
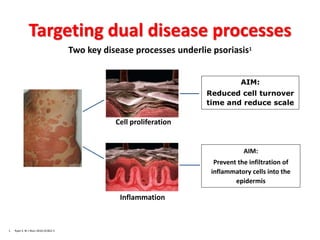
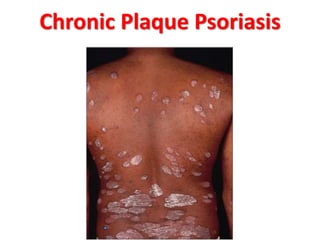
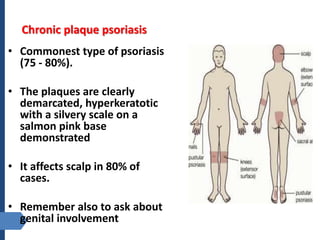
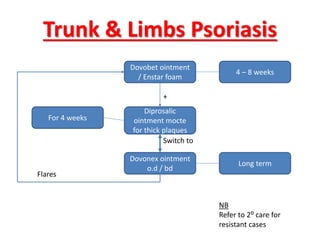
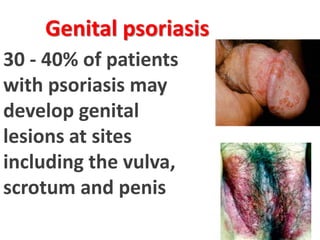
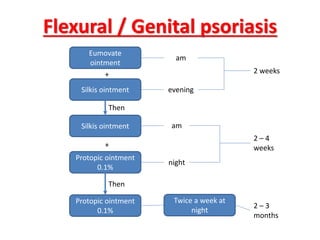
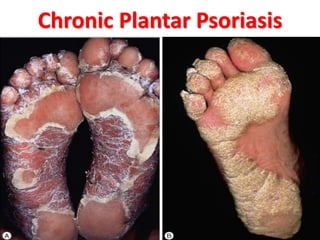
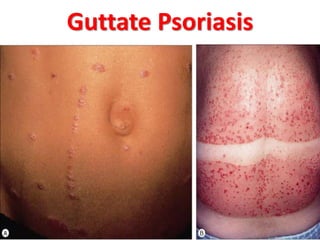
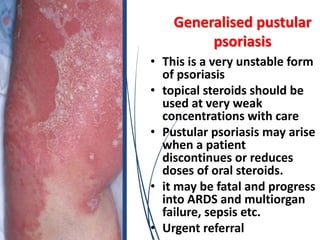
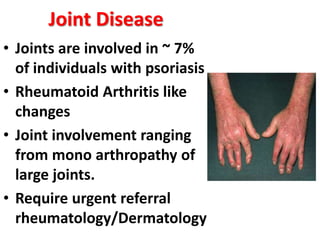
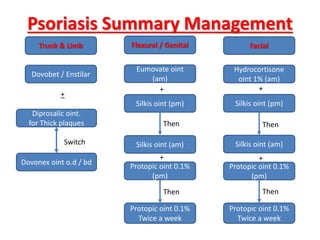
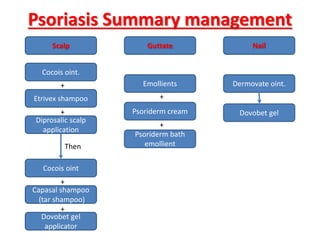
Psoriasis is a chronic, inflammatory skin condition characterized by red, scaly plaques. It has various clinical presentations including plaque, guttate, pustular, and erythrodermic forms. Treatment involves targeting the dual processes of inflammation and rapid skin cell turnover, using topical agents for mild disease and phototherapy or systemic drugs for more severe cases. Management requires a personalized approach considering disease characteristics and patient factors.