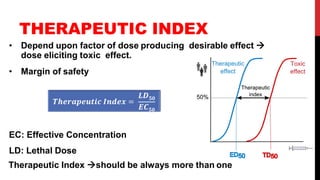
This document provides an overview of pharmacodynamics, which is the study of how drugs act on the body. It discusses key topics including:
- Mechanisms of drug action like agonism, antagonism, and efficacy
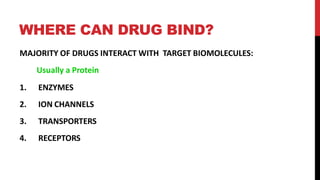
- Where drugs can bind in the body, primarily enzymes, ion channels, transporters, and receptors
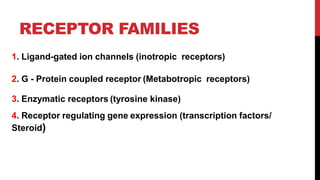
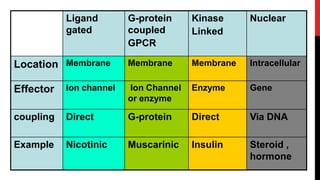
- The four main families of receptors - ligand-gated ion channels, G-protein coupled receptors, enzymatic receptors, and nuclear receptors
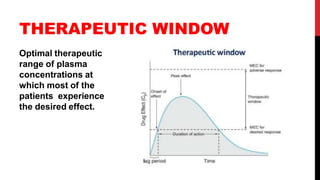
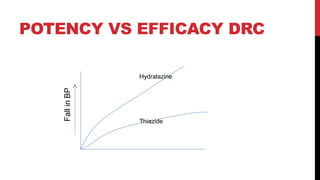
- Concepts of dose response relationships, therapeutic indices, and the development of drug tolerance over time.
In summary, the document outlines fundamental principles of pharmacodynamics and how drugs interact with the body at a molecular level.



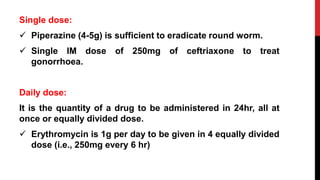
![DOSE RESPONSE CURVE
Emax X [D]
E =
Kd + [D]
dose
%response
100% -
50% -
Log dose%response
100% -
50% -
Saturation of Receptors](https://image.slidesharecdn.com/principlesofpharmacodynamics-200729095345/85/Principles-of-pharmacodynamics-22-320.jpg)








































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














