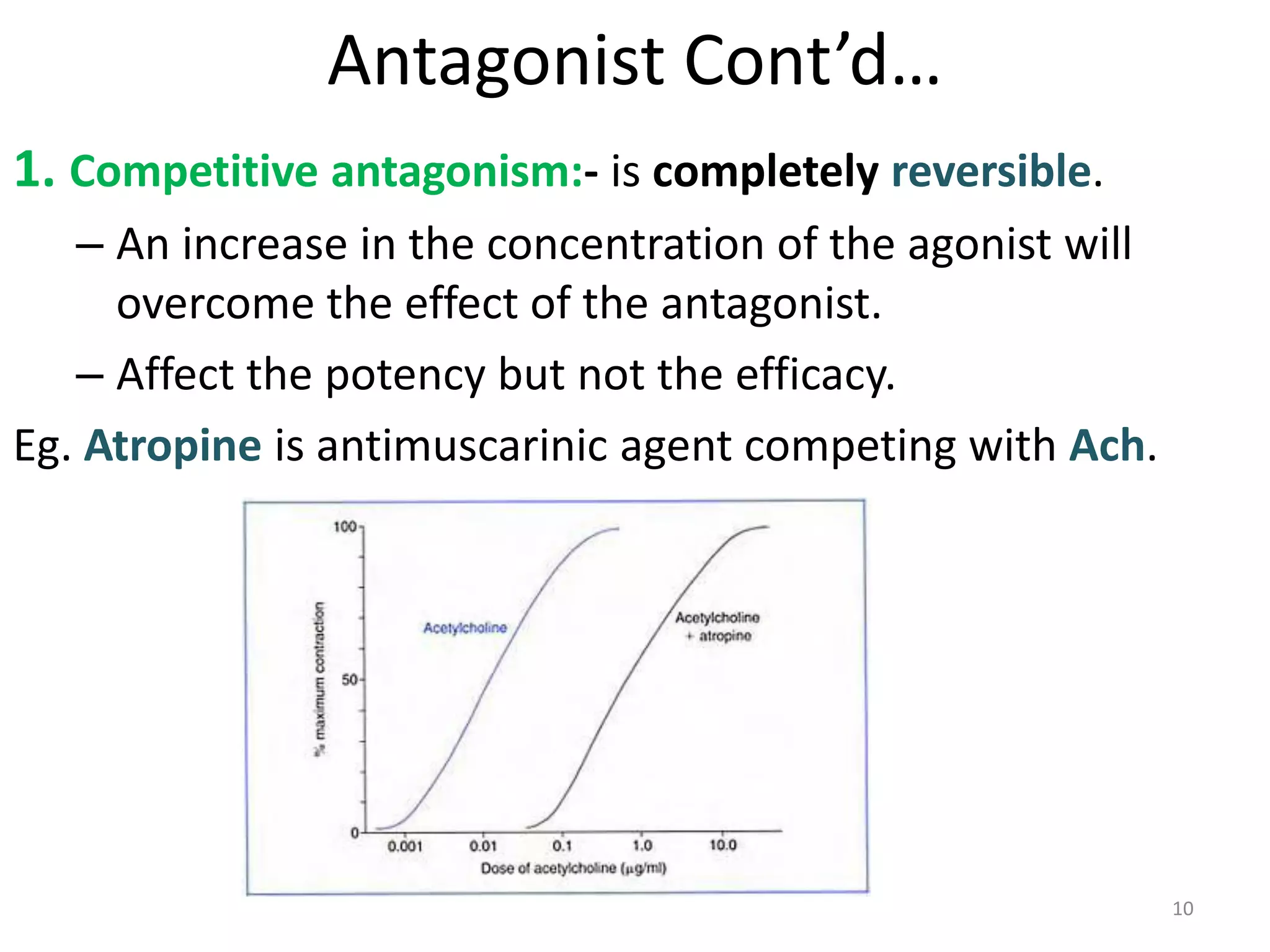
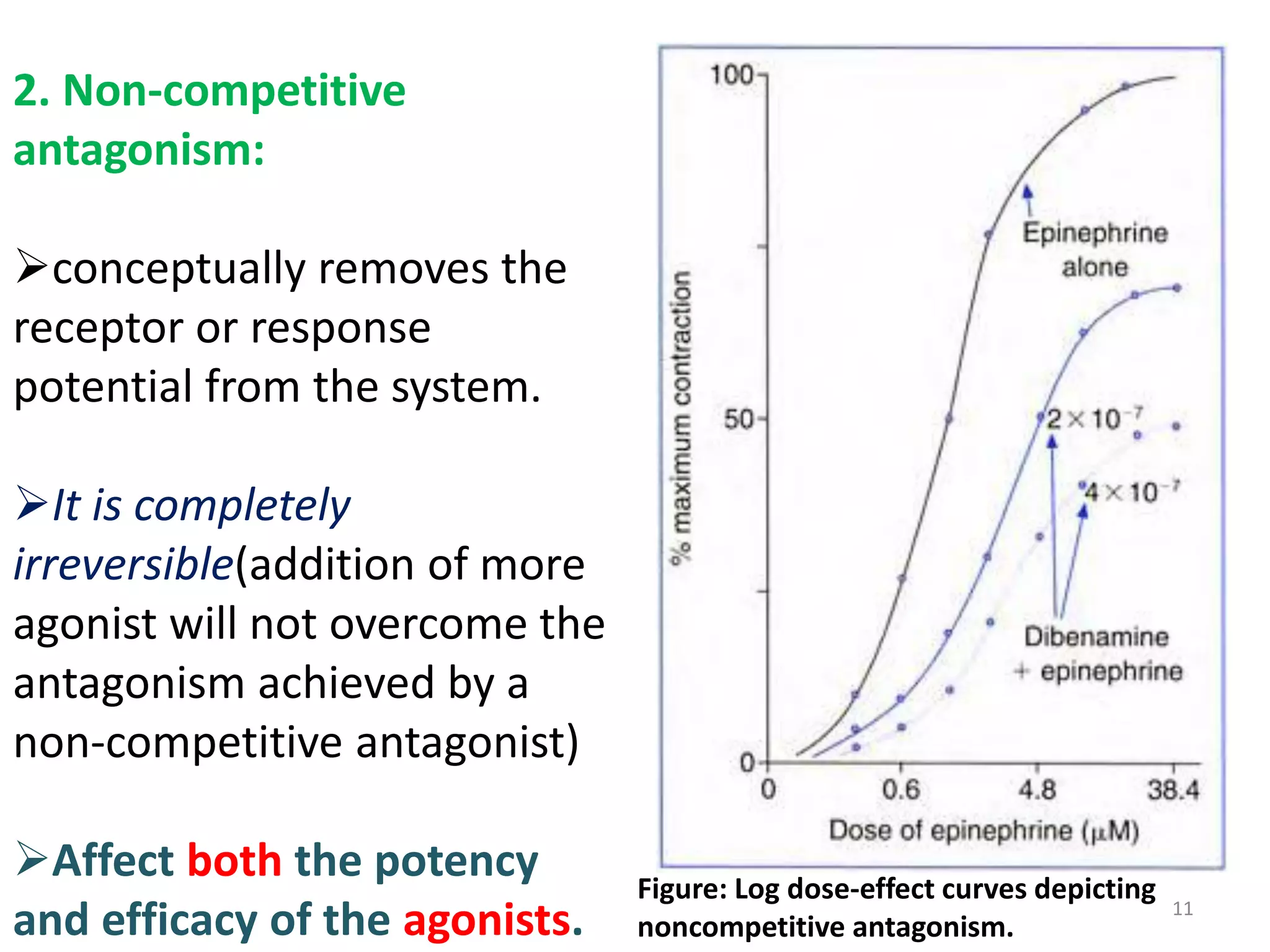
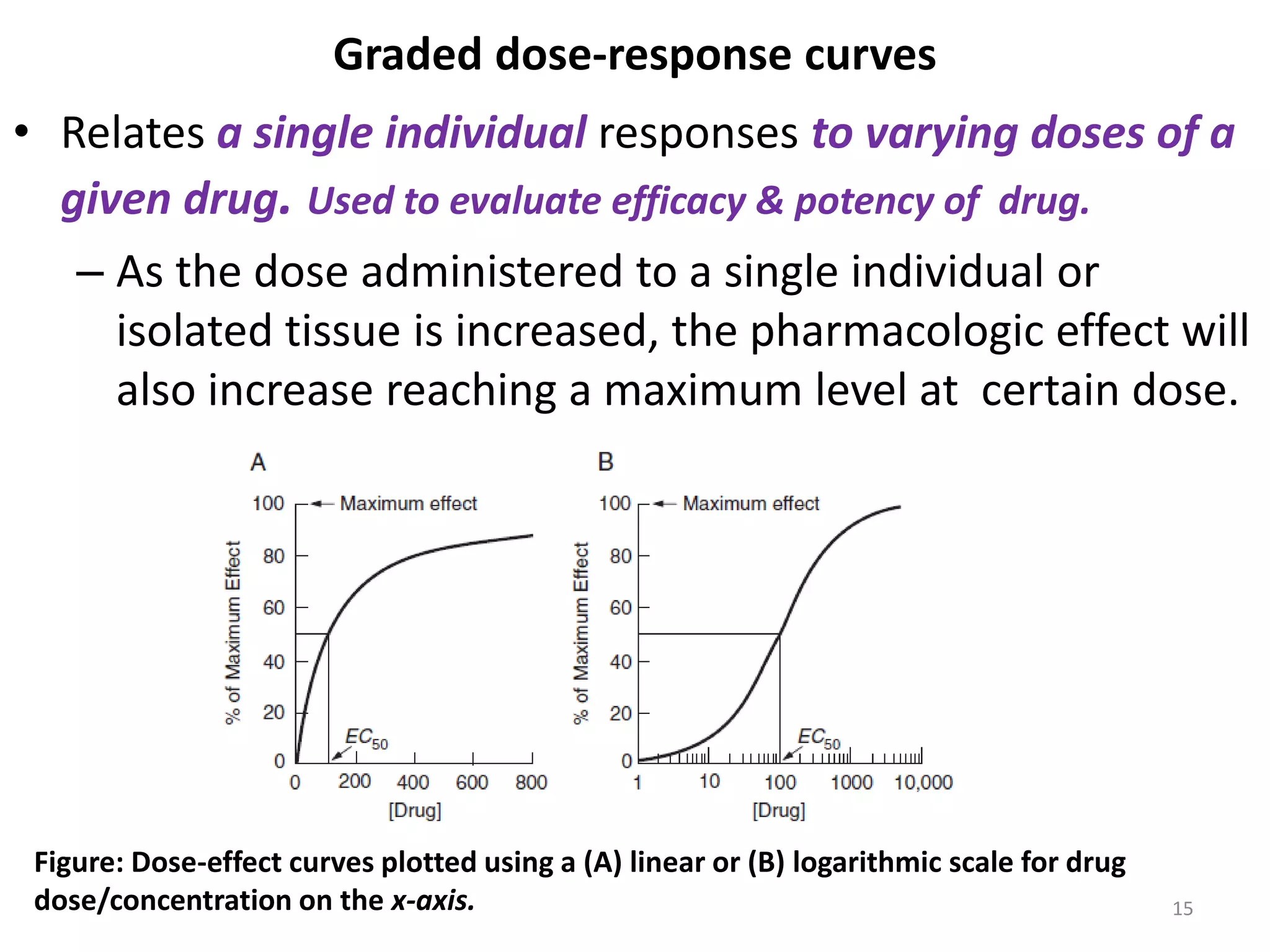
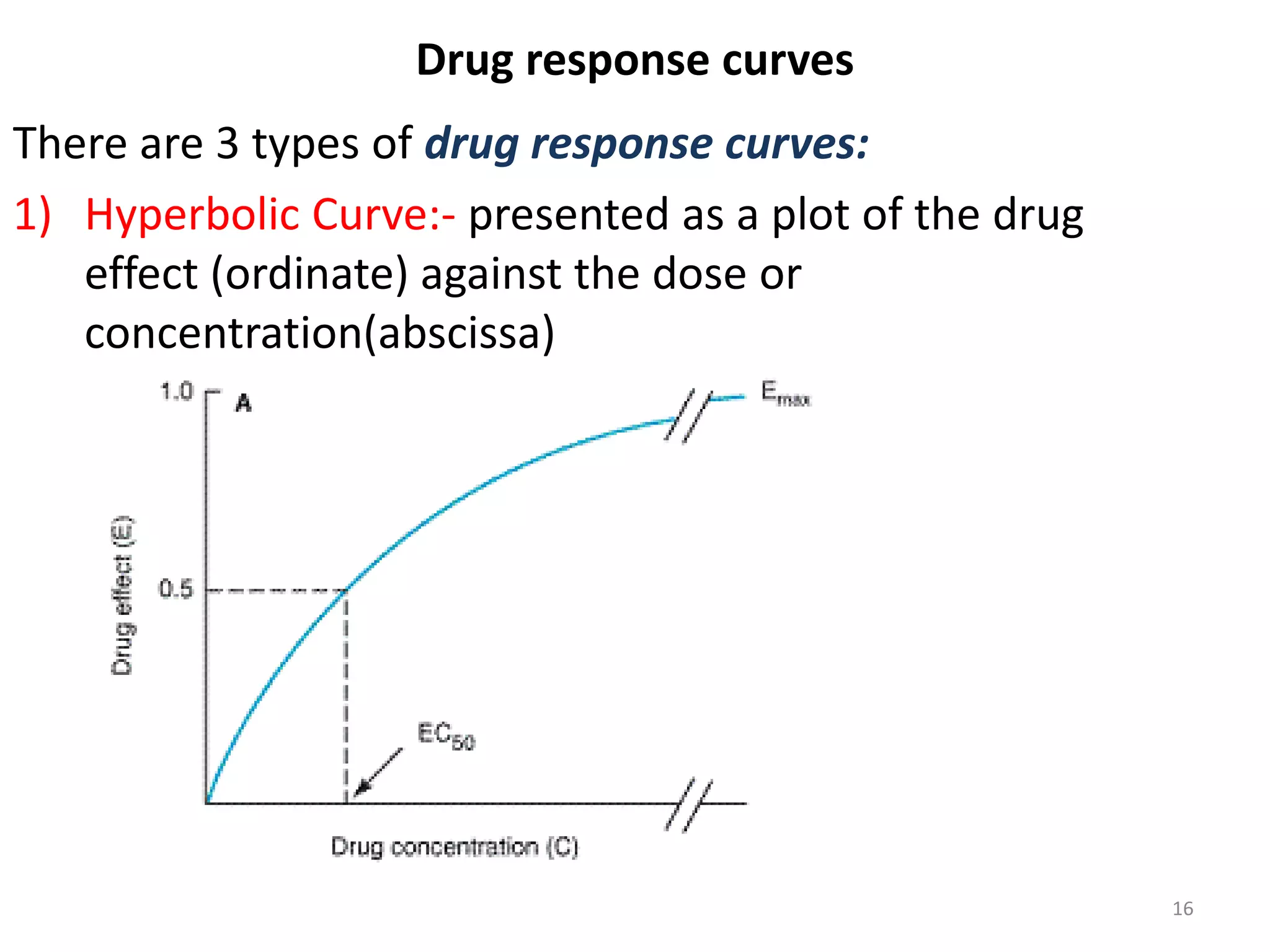
Pharmacodynamics deals with the biochemical and physiological effects of drugs and their mechanisms of action. Drugs act through receptor-mediated or non-receptor mediated pathways. Most drug receptors are proteins that determine drug action selectivity and response. Drug-receptor binding results in a response. Efficacy refers to the maximal response a drug can produce while potency is the dose required to produce a particular effect. Affinity is the tendency of a drug to bind receptors, while occupancy is the fraction of receptors bound. Agonists activate receptors to produce responses while antagonists inhibit agonist binding without efficacy. Dose-response relationships relate effect to dose and can be quantal or graded. Tolerance develops with repeated dosing due


































































![ABNORMAL LABOUR[]{}#%^*+=_\|~<>€£¥•.,?!’-/:(($$&@“.,?!’pdf](https://cdn.slidesharecdn.com/ss_thumbnails/abnormallabour-240814080030-7769169f-thumbnail.jpg?width=640&height=640&fit=bounds)
![PIHTN.pptx is increase of blood pressure during pregnancy of the mother [{}]#...](https://cdn.slidesharecdn.com/ss_thumbnails/pihtn-240806061903-454708ae-thumbnail.jpg?width=640&height=640&fit=bounds)
![Rh Alloimunization documents:;($&@“.,?!’[]{#%^*+=_\|~<€£¥•.,?!’](https://cdn.slidesharecdn.com/ss_thumbnails/rhalloimunization-240806061051-9740853c-thumbnail.jpg?width=640&height=640&fit=bounds)









![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)

















