Download to read offline
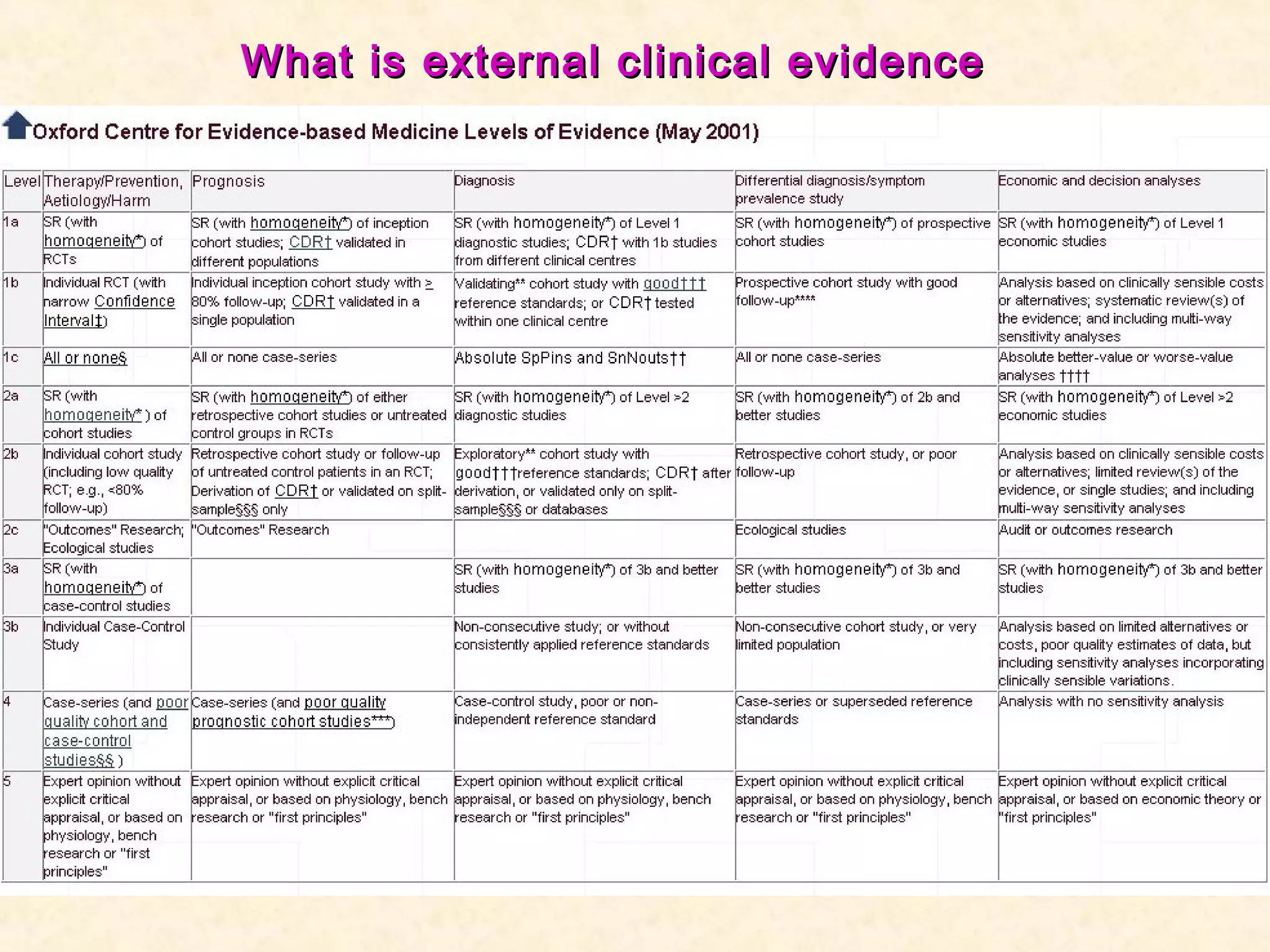
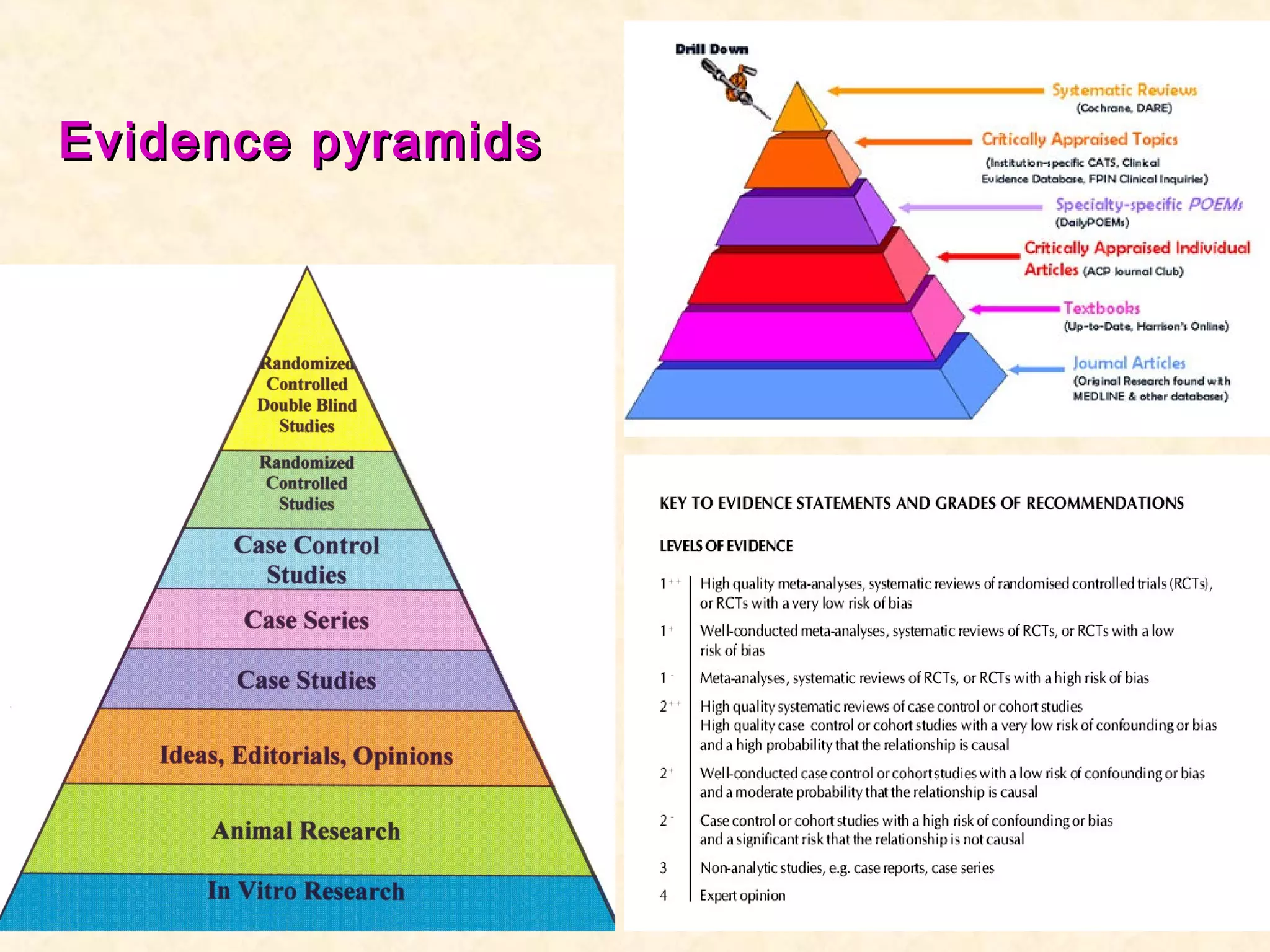



This document discusses evidence-based medicine and related concepts. It defines evidence-based medicine as the conscientious, explicit and judicious use of current best evidence in making decisions about patient care. It involves integrating individual clinical expertise with the best available external clinical evidence from systematic research. Medicine draws on both scientific knowledge and clinical expertise. While randomized controlled trials provide the strongest evidence, not all clinical questions can be answered through RCTs alone.































![Neurogenic bladder [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/neurogenicbladderedmond-140716213757-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)






























































