
Downloaded 97 times
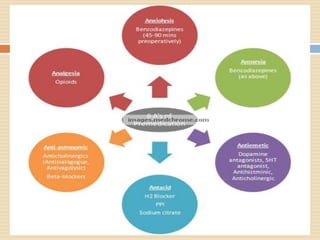

The document discusses preoperative medication and preparation of patients for anesthesia. It describes the goals of premedication as relieving anxiety, providing sedation, amnesia, analgesia and reducing surgical requirements. Common premedicant drug classes include benzodiazepines, opioids, anticholinergics and antiemetics. Ideal premedication has rapid onset, is safe and clears quickly without side effects. Factors like fasting, risk of aspiration and appropriate antibiotics are also covered.












































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)










