1) Nitrous oxide has been used as an anesthetic since the 1800s. It is commonly used today in combination with other anesthetic agents to reduce their required doses and decrease cardiovascular depression.
2) Nitrous oxide also has analgesic properties and is used for procedural sedation and pain management, though repeated or long-term use is discouraged due to health risks.
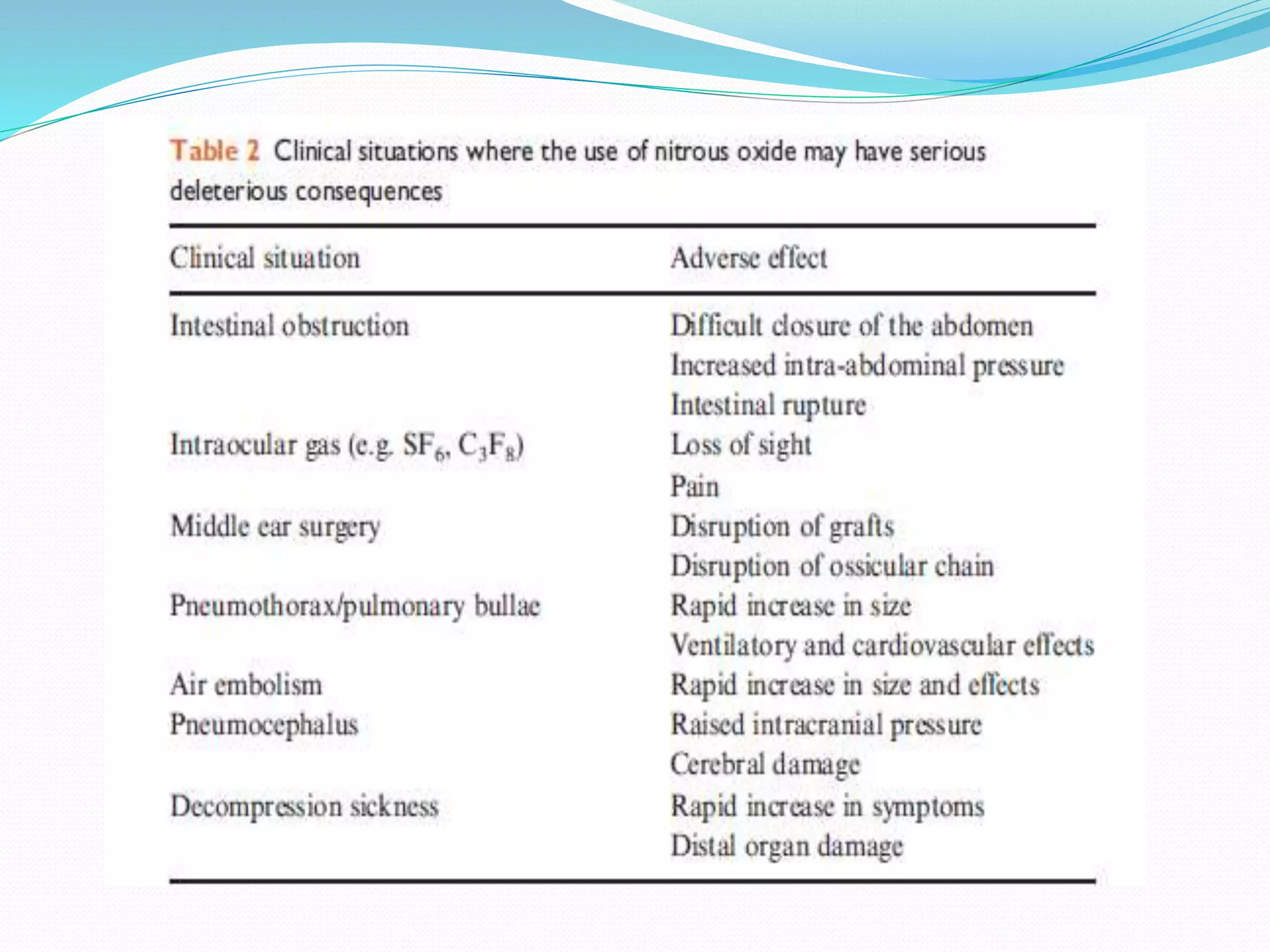
3) While nitrous oxide provides faster induction and recovery from anesthesia, its use may increase postoperative nausea and vomiting. Prolonged exposure can also cause vitamin B12 deficiency and neurological effects in some cases. Therefore, the risks and benefits must be considered when deciding whether to use nitrous oxide.