Download as PDF, PPTX



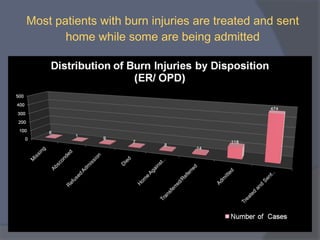
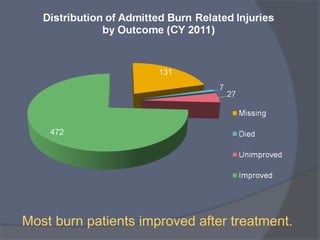
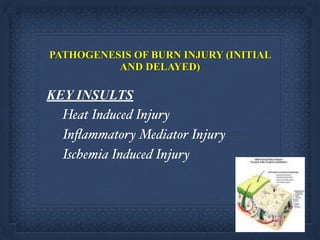
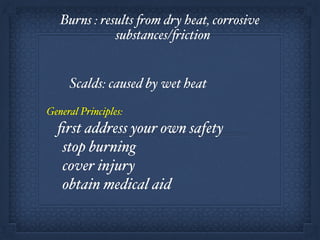

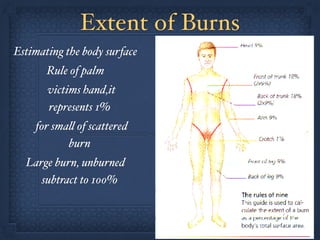
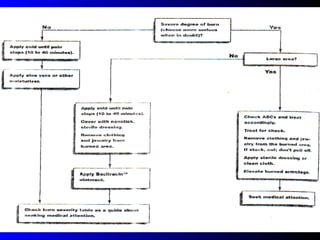
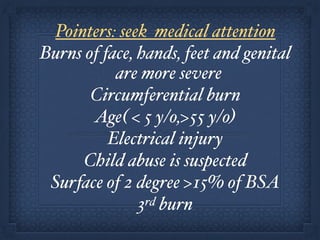
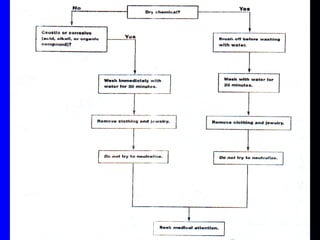
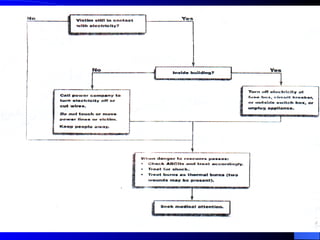
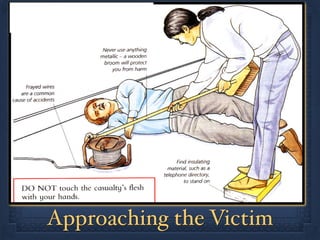
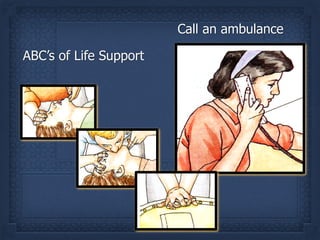
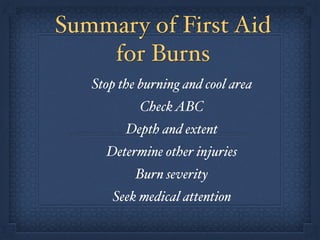
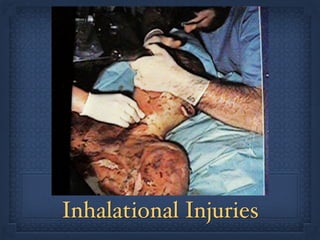


The document discusses burn injuries and their treatment. It notes that burns are a major global public health problem, causing over 195,000 deaths per year from fires alone. Burn treatment requires a multidisciplinary approach across various stages of care from first responders to long-term rehabilitation. The key types of burns are thermal, chemical, and electrical, with first aid including stopping the burn, assessing airway/breathing/circulation, and seeking prompt medical attention. Inhalation injuries can also occur and carbon monoxide poisoning is a leading cause of fire-related deaths. Proper first aid and emergency care is essential for burn patients.































































































