
Downloaded 24 times
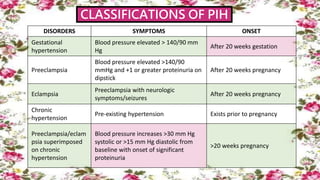
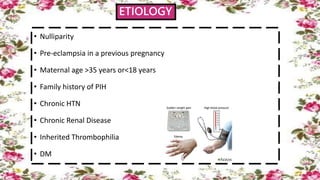
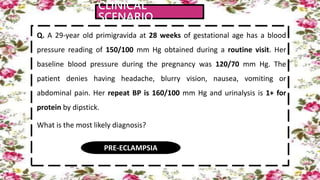













1) Pregnancy induced hypertension (PIH) refers to gestational hypertension, preeclampsia, and eclampsia that can occur during pregnancy. The document outlines the signs, symptoms, classifications, risk factors, management, and nursing responsibilities for PIH conditions. 2) Preeclampsia is diagnosed in a pregnant woman after 20 weeks gestation with new onset hypertension and proteinuria. Severe preeclampsia requires immediate delivery of the baby and mother. 3) Eclampsia occurs when a woman with preeclampsia experiences seizures in addition to her other symptoms. It is a medical emergency treated with magnesium sulfate and delivery of the baby.























































































