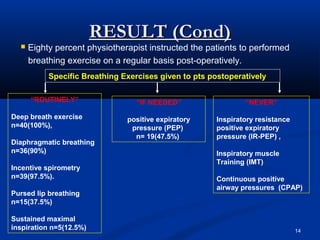
The document discusses a study that surveyed physiotherapists in Karachi, Pakistan about their chest physiotherapy practices for patients undergoing open heart surgery. Key findings included that physiotherapists commonly provide preoperative education and recommend postoperative breathing exercises. The most frequent techniques used were deep breathing without devices and incentive spirometry. Recommendations for continuing exercises after discharge varied. The study provides insight into chest physiotherapy awareness and techniques used among cardiothoracic physiotherapists in Karachi.