Downloaded 83 times













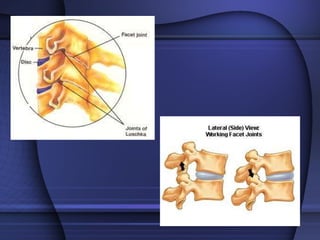






















The document discusses the anatomy and biomechanics of the cervical spine. It describes the seven cervical vertebrae, their characteristics, and motion segments. It also covers indications for cervical manipulation, mechanisms of action, and importance of screening for vascular risks prior to cervical manipulation.






































![MT-01 Anatomy and biomechanics of cervical spine-102024 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mt-01anatomyandbiomechanicsofcervicalspine-102024autosaved-250827121120-fd4fe0b6-thumbnail.jpg?width=640&height=640&fit=bounds)




























