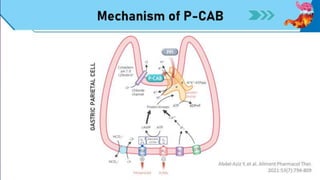
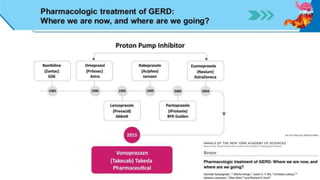
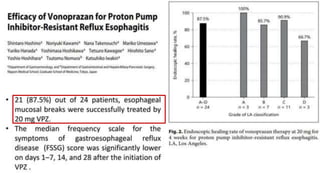
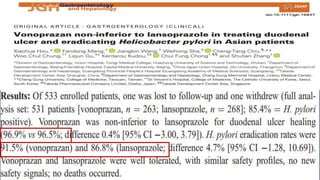
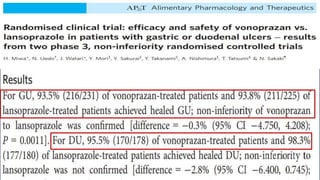
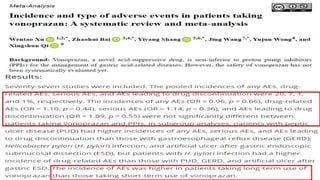
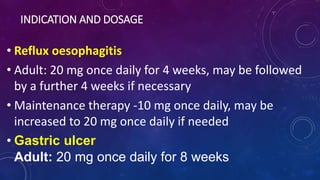
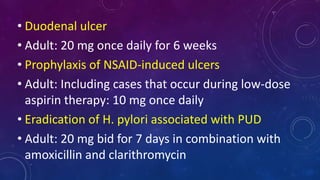
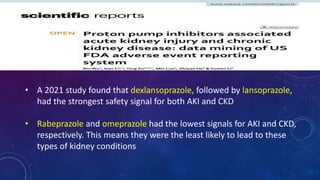
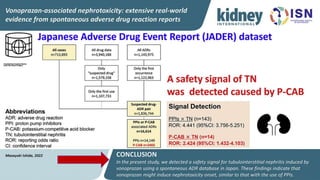
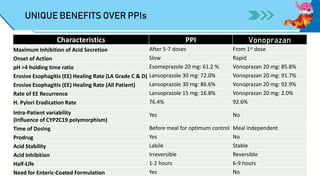
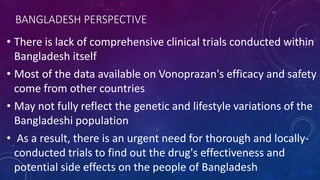
The document discusses potassium-competitive acid blockers (p-CABs) as innovative treatments for acid-related diseases, highlighting vonoprazan's advantages over traditional proton pump inhibitors (PPIs). It details vonoprazan's rapid onset, long duration, and effectiveness in treating conditions like erosive esophagitis and H. pylori eradication, while also acknowledging the limitations of existing PPI therapies. The document emphasizes the necessity for local clinical trials in Bangladesh to assess the drug's efficacy and safety in the regional population.