Download to read offline

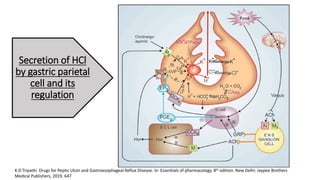
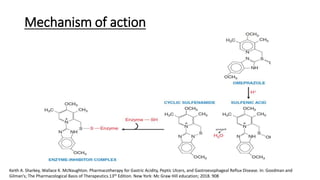
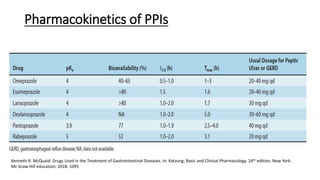
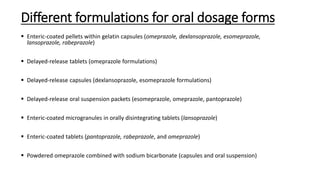
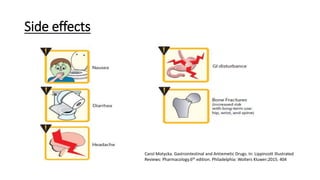



The document discusses the secretion of hydrochloric acid by gastric parietal cells and the regulation of drugs used to treat peptic ulcers and gastroesophageal reflux disease, specifically proton pump inhibitors (PPIs). It highlights various formulations, therapeutic uses, potential side effects, and drug interactions related to PPIs like omeprazole, lansoprazole, and pantoprazole. Additionally, it covers considerations for patients with renal and hepatic diseases regarding PPI dosage and effectiveness.























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)











