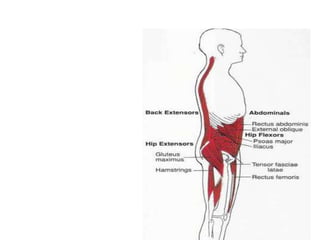
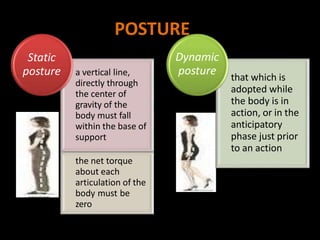
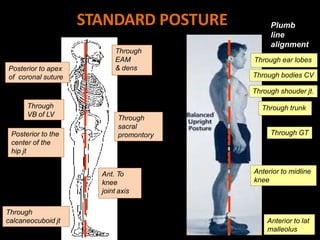
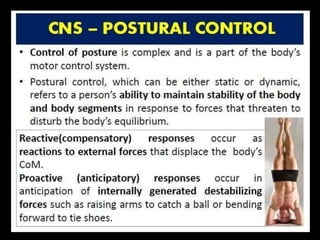
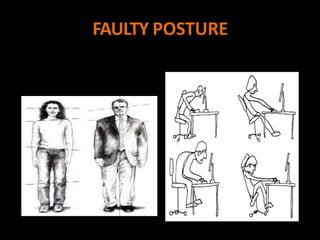
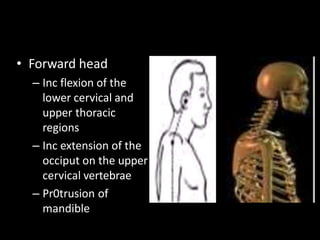
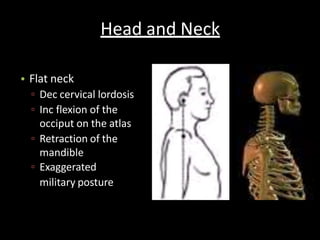
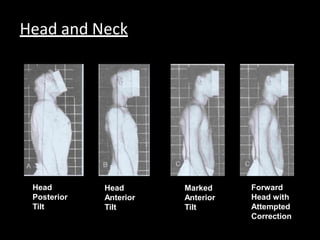
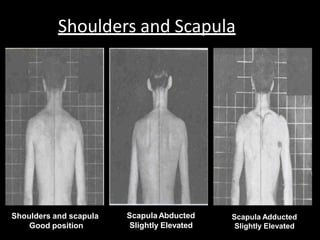
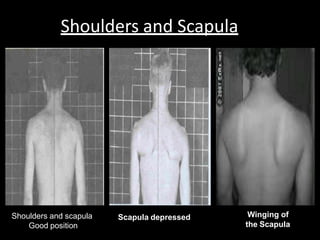
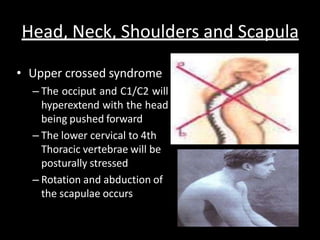
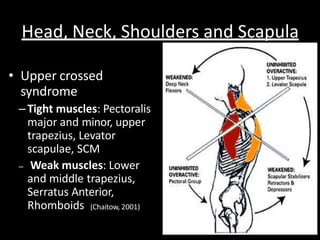
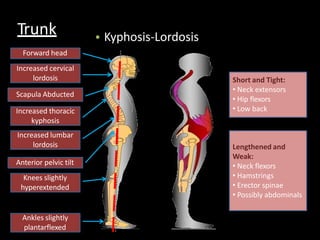
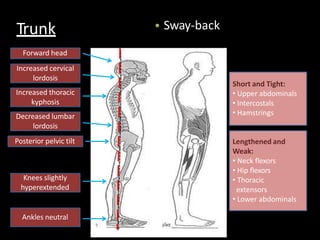
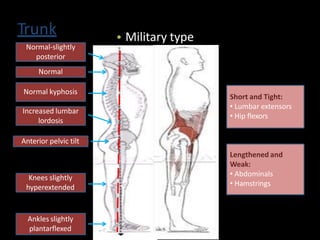
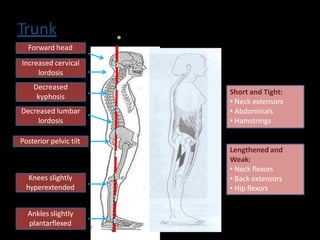
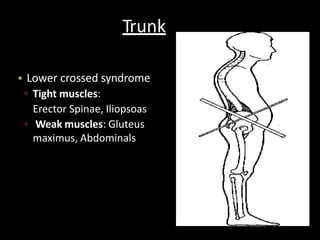
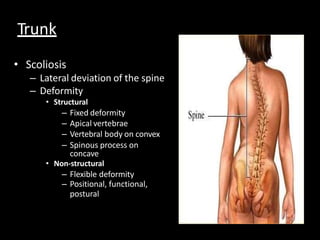
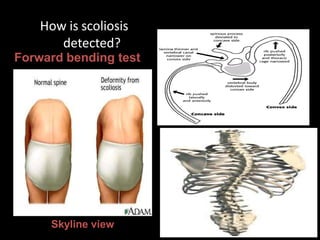
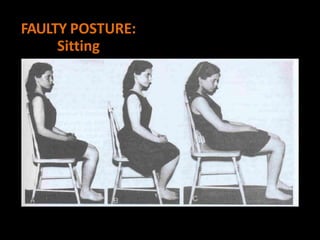
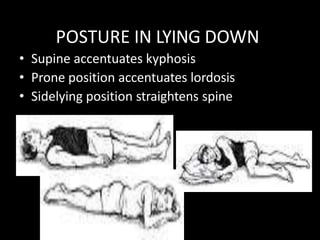
This document defines and describes different types of posture including static, dynamic, and ideal posture. It explains that posture results from the interaction of muscles, bones, and ligaments working together. Static posture maintains a constant position while dynamic posture adjusts with movement. Ideal posture minimizes strain and maximizes support. The document then describes common faulty postures involving the head, neck, shoulders, trunk, and pelvis. It details how different muscle imbalances can lead to issues like forward head, sway back, military-type posture, and lower crossed syndrome. The document also discusses scoliosis and how it is detected.






























![CyberLink PhotoDirector Ultra Crack Free Download [Latest] 2025](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409211238-0f15f8fb-thumbnail.jpg?width=640&height=640&fit=bounds)

![Freemake Video Converter Crack + Serial Key [Latest]](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409205402-3ea828f6-thumbnail.jpg?width=640&height=640&fit=bounds)

![Waves Ultimate 15 v24.11.17 With Crack for MacOS [Latest ]](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409210017-8d703091-thumbnail.jpg?width=640&height=640&fit=bounds)































