Posture
Posture is theattitude which is assumed
by body parts to maintain stability and
balance with minimum effort and least
strain during supportive and non
supportive positions.
Standing Posture (ErectPosture)
Although the COG in normal standing posture
is relatively high and presence of a narrow
base of support (both feet width and length)
only a minimal activity of muscular
contraction is required in maintenance of
static standing posture
?
What is the reason of it
?
5.
Factors affecting mechanicsof
posture
:
1-Body Physique. Body build i.e. percentage
of fat free component (muscles and bones
to adipose tissue.)
2- Nervous Control of posture.
3- Pathway of line of gravity.
4- Pelvic Inclination.
6.
In normal optimalstanding posture the LOG falls
close to not through most joint axes. Which is
counterbalanced by passive tension produced by
ligaments and other soft tissues, joints reaction forces
in addition to active tension produced by minimal
muscular activity.
3-Normal pathway of line of gravity in static
standing posture:
7.
From frontal view
TheLOG passes through the body’s center of gravity
which theoretically bisects the body into two equal
halves, with the body weight is equally distributed
between the two feet
.
4- Anterior tothe axis of flex./ext. of the upper cervical:
Creating a flexion moment which is (counter balanced by
tension in ligamentum nuchae and activity of neck extensor
muscles, to keep head in neutral position.
5- Posterior to the cervical spine:
Thus creating extension moment.
6- At the junction of the cervico-dorsal vertebrae:
No moment.
7- Anterior to the body of the dorsal vertebrae: Thus creating
flexion moment.
10.
8- At thejunction of the dorso lumbar vertebrae:
No moment.
9- Posterior to the body of the lumbar vertebrae:
Thus creating extension moment. Counter balanced by anterior
longitudinal ligament of the spine.
10-Through 5th
lumbar vertebrae, and posterior to the junction of
the lumbosacral joint:
Thus creating extension moment. Counter balanced by anterior
longitudinal ligament of the spine.
11.
11-Anterior to sacroiliacjoint:
Thus creating flexion moment (which tends to
cause the superior portion of the sacrum to
rotate anteriorly and inferiorly and the inferior
portion of the sacrum to rotate in the posterior
direction). Counter balanced by sacrospinous
and sacrotuberous ligaments. In addition to the
sacroiliac ligament which counter balance the
anterior rotation of the upper sacrum.
13.
12-Just behind (throughgreater trochanter) or via the axis of the
hip joint:
Thus may create extension moment which tends to rotate pelvis
posteriorly on the femoral head. So counterbalanced by
illiopsoas muscle activity and iliofemoral, pubofemoral and
ischiofemoral ligaments.
13- Anterior to the axis of knee joint:
Thus may create extension moment (stabilizing).
Counterbalanced by passive tension in posterior joint capsule
and associated ligaments to prevent hyperextension of knee
joint.
14- 5 cm (2 inches) in the front of the ankle joint at the level of the
tarsal bones:
Creates a dorsiflexion moment counter balanced by calf
muscles to prevent forward motion of tibia.
15.
Changes in NormalLOG Pathway
• If a subject is carrying a mass or a pregnant woman
so LOG moves further anteriorly and there will be
a tendency to fall forward. Counterbalanced by
activities of back extensors.
• If a subject climbs a hill the LOG falls backward,
so the person will move forward to counterbalance
this action. So he shifts the LOG forward and
keeps it within the base of support.
16.
• If asubjects descends a hill, the COG falls in front
of him so he will move the trunk backward with
increase in the lumbar lordotic curve to counteract
the effect of gravity.
• In case of wearing high heeled shoes in normal
standing position, the LOG moves forward more
than usual and thus increase load on calf muscles.
17.
Role of Globaland Core Muscle Activity
The muscles of the neck and trunk not only act as prime movers or
as antagonists to movement caused by gravity during dynamic
activity, they are important stabilizers of the spine
.
Without the dynamic stabilizing activity from the trunk muscles, the
spine would collapse in the upright position
.
Both superficial (global) and deep (core) muscles function to
maintain the upright posture
.
The global muscles are the large guy wires that respond to
external loads imposed on the trunk that shift the center of mass
.
18.
Their reaction isdirection-specific to control spinal
orientation
.
The global muscles are unable to stabilize individual spinal
segments except through compressive loading because
they have little or no direct attachment to the vertebrae
.
If an individual segment is unstable, compressive loading
from the global guy wires may lead to or perpetuate a
painful situation as stress is placed on the inert tissues at
the end of the range of that segment
20.
The deeper, coremuscles, which have segmental
attachments, respond regardless of direction of motion
.
They provide dynamic support to individual segments in
the spine and help maintain each segment in a stable
position so the inert tissues are not stressed at the
limits of motion
.
Both the global and core musculature play critical roles in
providing stability to the multi-segmental spine
.
21.
Role of MuscleEndurance
Only about 10% of maximum contraction is needed to provide
stability in usual situations
.
Slightly more might be needed in a segment damaged by disk
disease or ligamentous laxity when muscles are called on to
compensate for the deficit in the passive support
.
More type I fibers in back muscles making them more of
stabilizing tissues
.
Inactivity changes muscle fiber composition and is said to be
the reason of decreased activity in LBP patients
.
22.
Muscle Control inthe Lumbar
Spine
• TrAbd and Multifidi provide segmental control
and stiffness.(local stabilizers)
• First muscles to get active in case of postural
disturbance from rapid extremity movements.
• Intersegmental muscles and deep fibers of the
quadratus lumborum.
Postural Evaluation
• HyperlordoticPosture:
– Joints involved:
• Lumbar spine, pelvis, hip
– Possible cause:
• Tightened or shortened hip flexor muscles
• Weakened or elongated hip extensors or
abdominals
• Poor postural sense
– Adverse effects:
• ↑ lumbar lordosis
• Anterior pelvic tilt
• Hips assuming a flexed position
25.
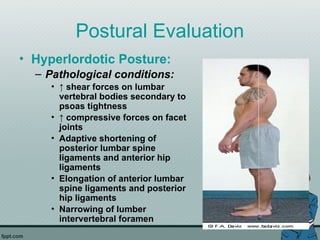
Postural Evaluation
• HyperlordoticPosture:
– Pathological conditions:
• ↑ shear forces on lumbar
vertebral bodies secondary to
psoas tightness
• ↑ compressive forces on facet
joints
• Adaptive shortening of
posterior lumbar spine
ligaments and anterior hip
ligaments
• Elongation of anterior lumbar
spine ligaments and posterior
hip ligaments
• Narrowing of lumber
intervertebral foramen
26.
Postural Evaluation
• KypholordoticPosture:
– Similar to hyperlordotic posture:
• ↑ total lumbar lordosis
– Differences:
• Compensatory ↑ in thoracic kyphosis:
– Attempt to maintain spine in position of equilibrium
• Cervical spine: ↑ in lordosis (Forward head
posture)
– Joints involved:
• Pelvis, hip joint, lumbar spine, thoracic spine,
cervical spine
27.
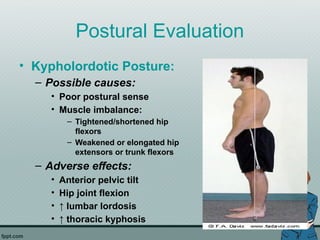
Postural Evaluation
• KypholordoticPosture:
– Possible causes:
• Poor postural sense
• Muscle imbalance:
– Tightened/shortened hip
flexors
– Weakened or elongated hip
extensors or trunk flexors
– Adverse effects:
• Anterior pelvic tilt
• Hip joint flexion
• ↑ lumbar lordosis
• ↑ thoracic kyphosis
28.
Postural Evaluation
• KypholordoticPosture:
– Pathological conditions:
• Adaptive shortening of
anterior chest muscles
• Elongation of thoracic
paraspinal muscles
• ↑ compressive forces on
anterior thoracic vertebrae and
posterior lumbar vertebrae
• ↑ tensile forces on
ligamentous structures in
posterior thoracic spine and
anterior lumbar spine
• ↑ facet joint compression
• Forward head posture
• Forward shoulder posture
30.
Postural Evaluation
• SwaybackPosture:
– Key: ↑ reliance on ligaments for postural stability
• Joints at end ROM (excessive stress on ligaments)
– Joints involved:
• Knees, hips, lumbar spine, lower thoracic spine, cervical
spine
– Possible causes:
• Ectomorph body: hypomobility of joints
• Poor postural sense
• Tightened/shortened hip extensors
• Weakened or elongated hip flexors or lower abdominals
• ↓ general muscular strength
31.
Postural Evaluation
• SwaybackPosture:
– Adverse Effects:
• Genu recurvatum
• Hip joint extension
• Posterior pelvic tilt
• Lumbar spine in neutral
or minimal flexed
position
• ↑ in lower thoracic,
thoracolumbar curvature
32.
Postural Evaluation
• SwaybackPosture:
– Pathological Conditions:
• Elongated or ↑ tensile forces
on anterior hip ligaments
and posterior aspect of
lower thoracic spine
• Adapted/shortened or ↑
compressive forces on
posterior hip ligaments and
anterior lower thoracic spine
• ↑ tensile force on posterior
knee and compressive force
on anterior knee
• ↑ shearing forces on L5/S1
• Forward head and shoulder
posture
33.
Postural Evaluation
• FlatBack Posture:
– Key: Lost normal “S” shape spine curvature in
the sagital plane
– Joints:
• Hip joint, lumbar spine, thoracic spine, cervical spine
– Possible causes:
• Shortened/tightened hip extensors, abdominal
musculature
• Weakened, elongated hip flexors
• Poor posture
– Adverse effects:
• Extended hip joint / posterior pelvic tilt
• Extended thoracic spine
• Flexed middle and lower cervical spine, extended upper
cervical spine
34.
Postural Evaluation
•
Flat BackPosture
:
Pathological conditions:
Compressive forces in
posterior hip joint, anterior
lumber and mid-low cervical
spines, posterior thoracic
and upper cervical spines
Elongation of soft tissue
Forward head posture
(compensation for posterior
spine displacement)
35.
Postural Evaluation
Scoliosis:
– Lateralcurvature of
spinal column
– Right handed people:
mild R thoracic L
lumbar S curve.
– May b asymmetry in hip
pelvis and lower
extremities.
36.
Muscle impairments
:
• Mobilityimpairment in structures on the concave side of the
curves.
• Impaired muscle performance due to stretch and weakness in
the musculature on the convex side of the curves.
• If one hip is adducted, the adductor muscles on that side have
decreased flexibility and the abductor muscles are stretched
and weak. The opposite occurs on the contralateral extremity.
• With advanced structural scoliosis, cardiopulmonary
impairment may restrict function.
37.
• Functional/ postural:
spineattempts to
compensate to
maintain the head in a
neutral position and
keep eyes level
• Reversible, changes
with forward bending,
side bending and
positional changes.
– Muscular imbalance,
spasm, pelvic
obliquity, limb-length
discrepancy
• Structural: defect or congenital
bony abnormality of vertebrae
– Neuromuscular diseases
or disorders (e.g., cerebral
palsy, spinal cord injury,
progressive neurological
or muscular diseases),
– osteopathic disorders
(e.g., hemivertebra,
osteomalacia, rickets,
fracture).
Postural Evaluation
• ForwardShoulder Posture:
– Key: characterized by
protraction and elevation of
scapulae and a forward,
rounded position of
shoulders
• May include scapula winging
and IR
• Forward head posture
– Joints:
• Scapulothoracic articulation
• Glenohumeral joint
• Thoracic spine
• Cervical spine
40.
Postural Evaluation
• ForwardShoulder
Posture:
– Possible causes:
• Tightened, shortened pectoral
muscles
• Weakened or elongated
scapular retractors (mid and
low trapezius, rhomboids)
• Poor postural awareness
and/or muscle fatigue
• Large breast development
– Adverse effects:
• Humeral head stress
(displaced anteriorly)
• Forward head posture
Postural Evaluation
• ScapulaWinging:
– Weakness of
serratus anterior,
middle and lower
trapezius
• Long thoracic
nerve
– Biomechanics of
normal arm
movement thrown
off
43.
Postural Evaluation
• ForwardHead Posture:
– Key: anterior displacement
of head relative to thorax
– Joints:
• Cervical spine, GH, thoracic
spine
– Possible causes:
• Poor eyesight (need glasses)
• Muscle fatigue/weakness
• Poor postural sense
– Adverse effects:
• Flexion of lower cervical spine
• Flattening of mid cervical spine
• GH motion affected
Leg length discrepancy
:
•An elevated ilium on the long leg (LL) side and lowered on the
short leg (SL) side is the characteristic deviation.
• This puts the LL side in hip adduction with greater shear stress
and the SL side in hip abduction with greater compression
stress.
• The sacroiliac (SI) joint on the LL side is more vertical with
greater shear stress; on the SL side it is more horizontal with
greater compression stress.
• Side bending of the lumbar spine toward the LL side coupled
with rotation in the opposite direction.
47.
• This compressesthe intervertebral disk on the LL side and
distracts the disk on the SL side; it also causes torsional stress.
• There is extension and compression of the lumbar facets on the
LL side (concave portion of the curve) and flexion and distraction
of the lumbar facets on the SL side (convex portion of the curve).
• There is narrowing of the intervertebral foramina on the LL side.
• The thoracic and cervical spine has compensatory scoliosis in
the opposite direction.
48.
Muscle Impairments
• Mobilityimpairment from decreased flexibility in the hip
adductors on the LL side and abductors on the SL side.
• Asymmetrical differences in the iliopsoas, quadratus
lumborum, piriformis, erector spinae, and multifidus
muscles, with those on the concave side of the curve or the
LL side having decreased flexibility.
• Impaired muscle performance from stretched and
weakened muscles including hip adductors on the SL side,
abductors on the LL side, and in general muscles on the
convex side of the curve.
49.
Sources of Symptoms
•Greater shear forces occur in the hip and SI joints on the LL side, which
increases stress in the supporting ligaments and decreases the load-bearing
surface in the joint.
• Degenerative changes occur more frequently in hips on the LL side.
• Stenosis in the lumbar intervertebral foramina on the LL cause vascular
congestion or nerve root irritation.
• Lumbar facet compression and irritation on the LL side.
• Disk breakdown from torsional and asymmetrical forces.
• Muscle tension, fatigue, or spasm in response to asymmetrical loading and
response.
• Lower extremity overuse syndromes.




















































![CyberLink PhotoDirector Ultra Crack Free Download [Latest] 2025](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409211238-0f15f8fb-thumbnail.jpg?width=640&height=640&fit=bounds)






![Waves Ultimate 15 v24.11.17 With Crack for MacOS [Latest ]](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409210017-8d703091-thumbnail.jpg?width=640&height=640&fit=bounds)

![Freemake Video Converter Crack + Serial Key [Latest]](https://cdn.slidesharecdn.com/ss_thumbnails/presentationonposture-250409203259-21999cb1-250409205402-3ea828f6-thumbnail.jpg?width=640&height=640&fit=bounds)

































