Pneumonia can be classified in several ways:
1. By anatomical region affected - lobar pneumonia involves an entire lung lobe while bronchopneumonia is patchy.
2. By where infection was acquired - community, healthcare, or ventilator associated.
3. By etiology - bacterial, viral, or other.
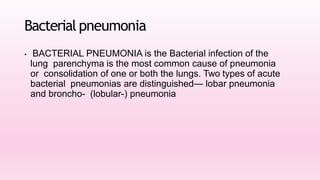
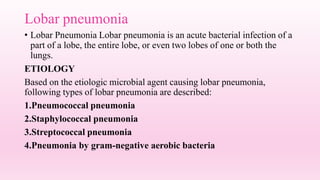
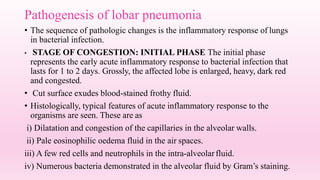
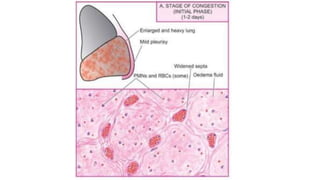
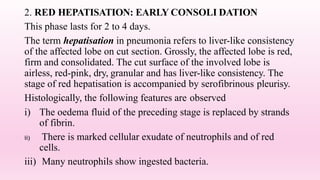
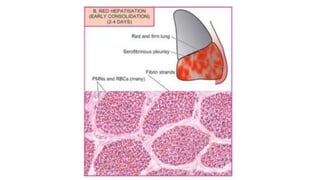
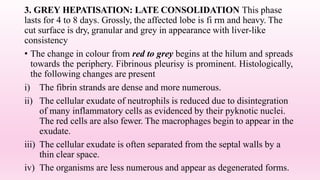
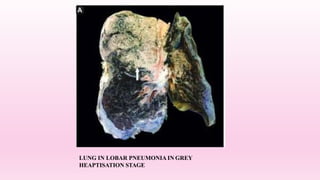
Bacterial pneumonia, the most common type, can be lobar or bronchopneumonia. Lobar pneumonia involves an inflammatory process over several days from congestion to red/grey hepatization and resolution. It typically has a sudden onset and is treated with antibiotics. Bronchopneumonia occurs in infants/elderly and shows patchy consolidation on x-ray.


































![Pulmonary_inections[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonaryinections1-230718060523-80803fef-thumbnail.jpg?width=640&height=640&fit=bounds)





































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)











