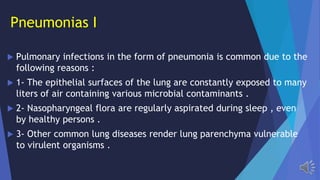
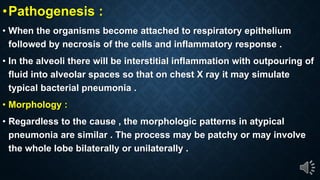
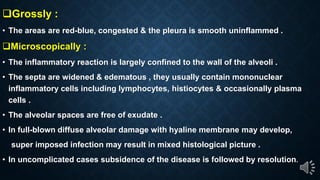
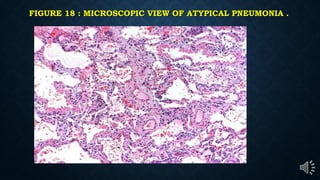
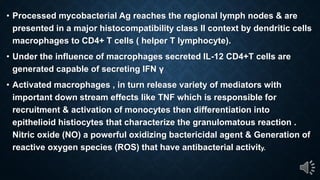
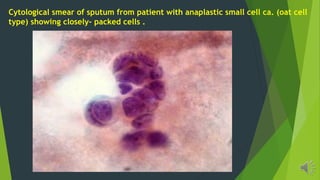
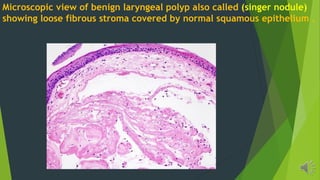
This document provides an overview of respiratory module part 2, covering pneumonia syndromes, lung carcinoma, pleural lesions, and nasopharyngeal and laryngeal carcinoma. It discusses community-acquired typical and atypical pneumonia caused by pathogens like Streptococcus pneumoniae, Haemophilus influenzae, and Mycoplasma pneumoniae. It describes the clinical presentation, pathology, and complications of bacterial and atypical pneumonias. It also briefly discusses SARS, MERS, and COVID-19 caused by coronaviruses.
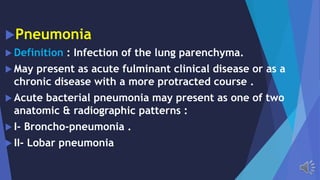
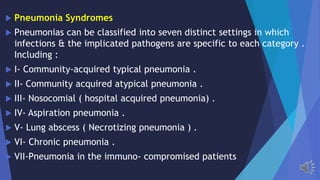



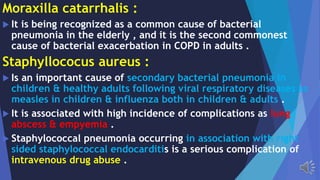


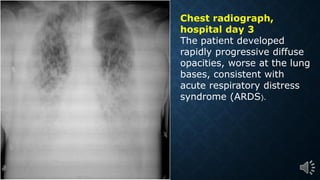
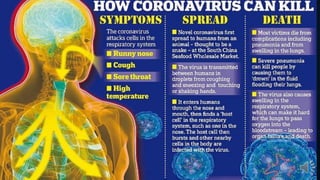
![If the air sacs then become inflamed, this causes an
outpouring of inflammatory material [fluid and inflammatory
cells] into the lungs and end up with pneumonia.
lungs that become filled with inflammatory material are
unable to get enough oxygen to the bloodstream, reducing
the body s ability to take on oxygen and get rid of carbon
dioxide.
That s the usual cause of death with severe pneumonia,](https://image.slidesharecdn.com/rspathology02-200606030148/85/Rs-pathology-02-55-320.jpg)
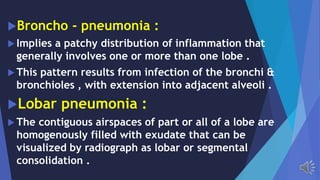
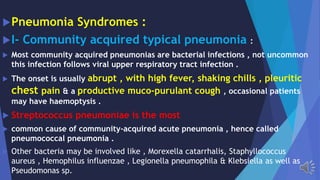
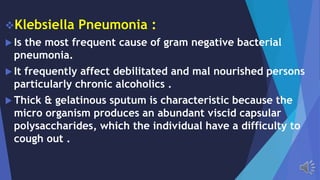
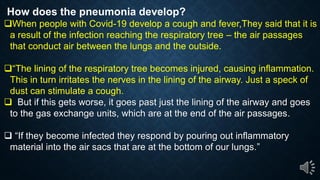
![IS COVID-19 PNEUMONIA DIFFERENT?
Covid-19 pneumonia is different from the most common cases that
people are admitted to hospitals for.
Most types of pneumonia that we know of and that we admit people to
hospital for are bacterial and they respond to an antibiotic. there is
evidence that pneumonia caused by Covid-19 may be particularly
severe. cases of coronavirus pneumonia tend to affect all of the lungs,
instead of just small parts.
Once we have an infection in the lung and, if it involves the air sacs,
then the body s response is first to try and destroy [the virus] and limit
its replication.](https://image.slidesharecdn.com/rspathology02-200606030148/85/Rs-pathology-02-57-320.jpg)






































![Pulmonary_inections[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pulmonaryinections1-230718060523-80803fef-thumbnail.jpg?width=640&height=640&fit=bounds)

































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


