Downloaded 34 times

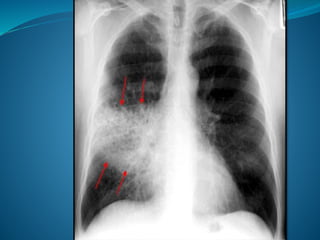


This document discusses respiratory tract infections, specifically pneumonia. It defines pneumonia as an acute inflammation of the lung parenchyma. Common causes are bacteria such as Streptococcus pneumoniae and viruses. Symptoms include fever, cough, chest pain, and breathlessness. Diagnosis involves chest x-ray, sputum and blood cultures. Treatment involves antibiotics, oxygen, hydration and nutrition. Nursing care focuses on airway clearance, breathing exercises, pain management and patient education.
















































































