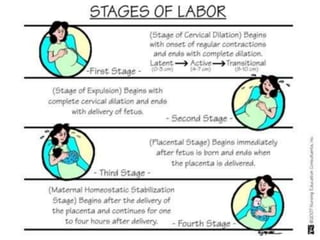
1. Labor is the process by which the viable products of conception are expelled from the uterus through the vagina. It involves uterine contractions and cervical dilation.
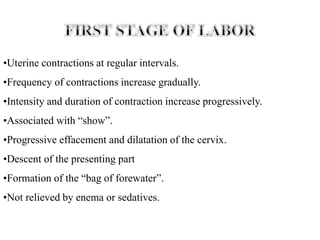
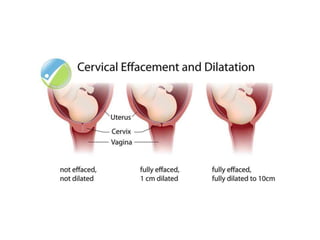
2. Nursing care during labor involves monitoring the patient, providing comfort measures, and preparing for delivery. The nurse assesses cervical dilation, fetal position, and signs of distress.
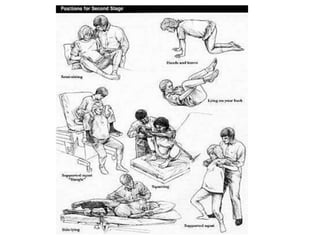
3. During the second stage of labor, nurses assist the patient in pushing effectively and maintaining an optimal birthing position. They provide encouragement and help the patient rest between contractions.