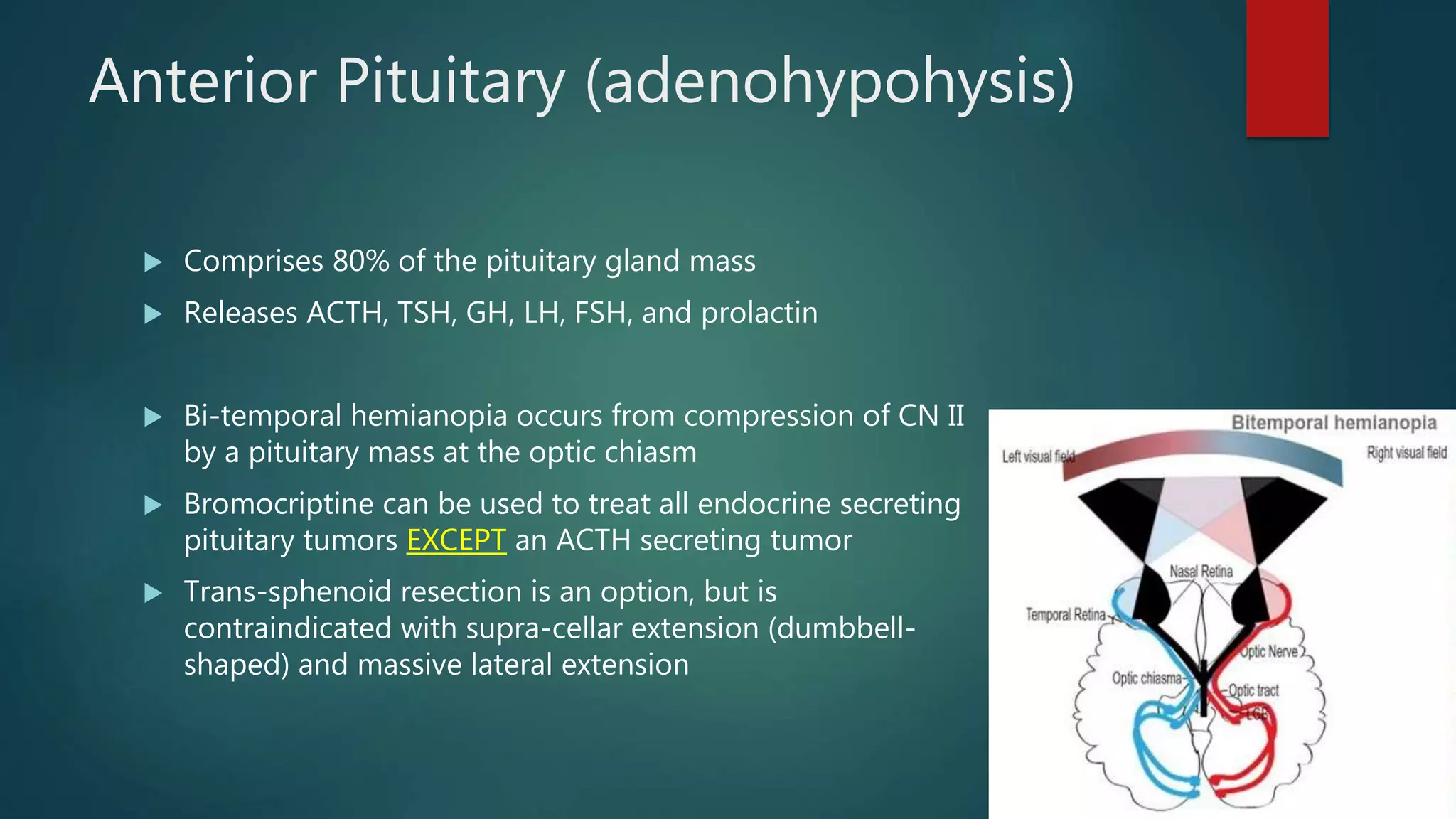
The document summarizes key information about the pituitary gland and adrenal glands. It discusses the anatomy and physiology of the pituitary gland and its role in controlling the anterior pituitary via hormones from the hypothalamus. It also discusses specific pituitary tumors like prolactinomas and acromegaly. It then covers the anatomy and physiology of the adrenal glands, including disorders like Cushing's syndrome, Conn's syndrome, adrenal insufficiency, and adrenal tumors. Evaluation and treatment of various pituitary and adrenal pathologies are summarized.