Objectives
Discuss the problemof maternal mortality
rates and its impact on the attainment of
MDG 5
Discuss interventions that are recommended
and are not recommended during:
o Antepartum
o Labor
o Delivery
o Immediate post-partum
BY: ROMMEL LUIS C. ISRAEL III 2
3.
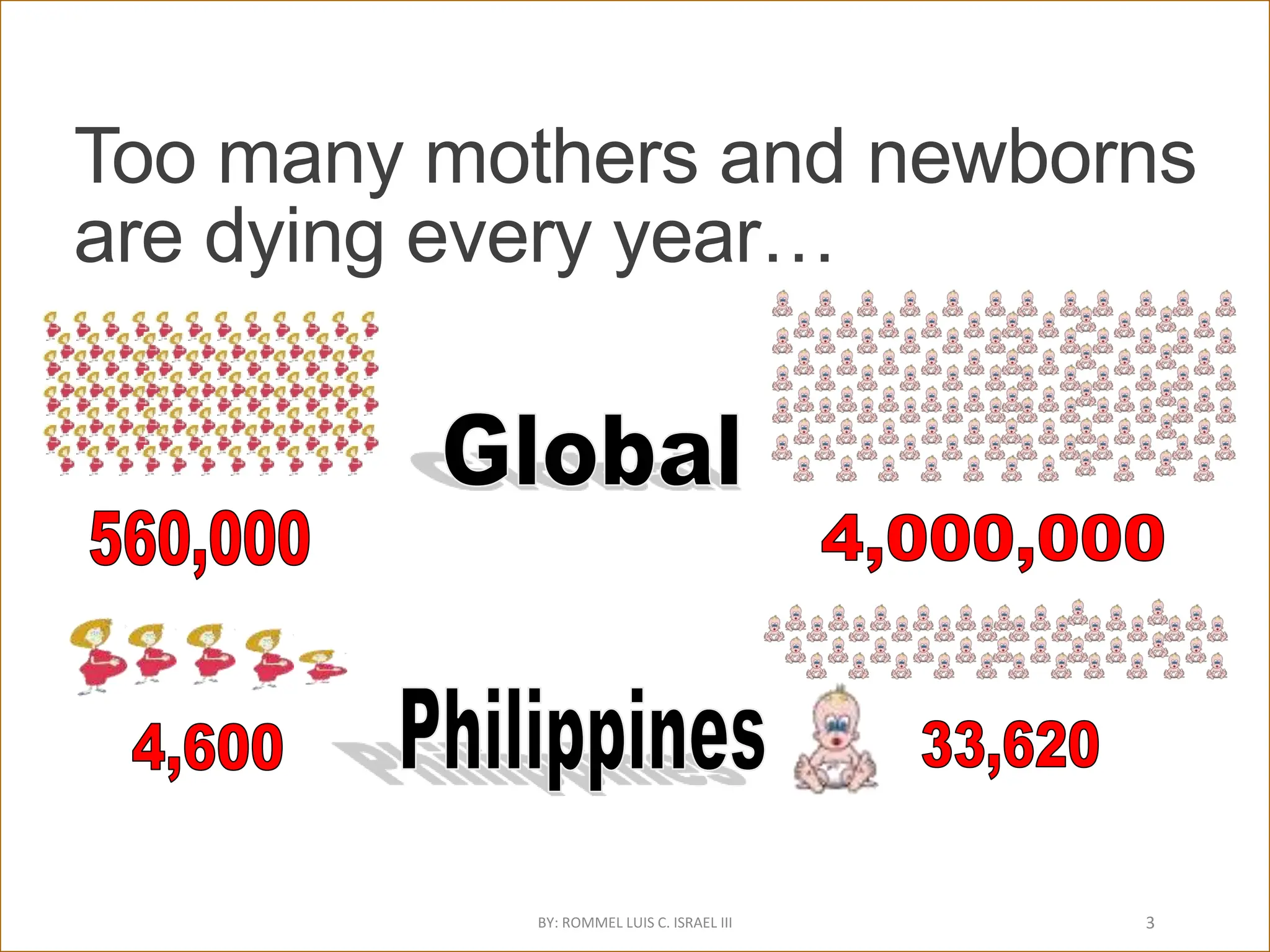
Too many mothersand newborns
are dying every year…
BY: ROMMEL LUIS C. ISRAEL III 3
4.
Most maternal deathsoccur during labor, delivery
and the immediate post-partum period
4
0-1 day 2-7 days 8-14 days 15-21 days 22-30 days 31-42 days
Day of maternal death after delivery
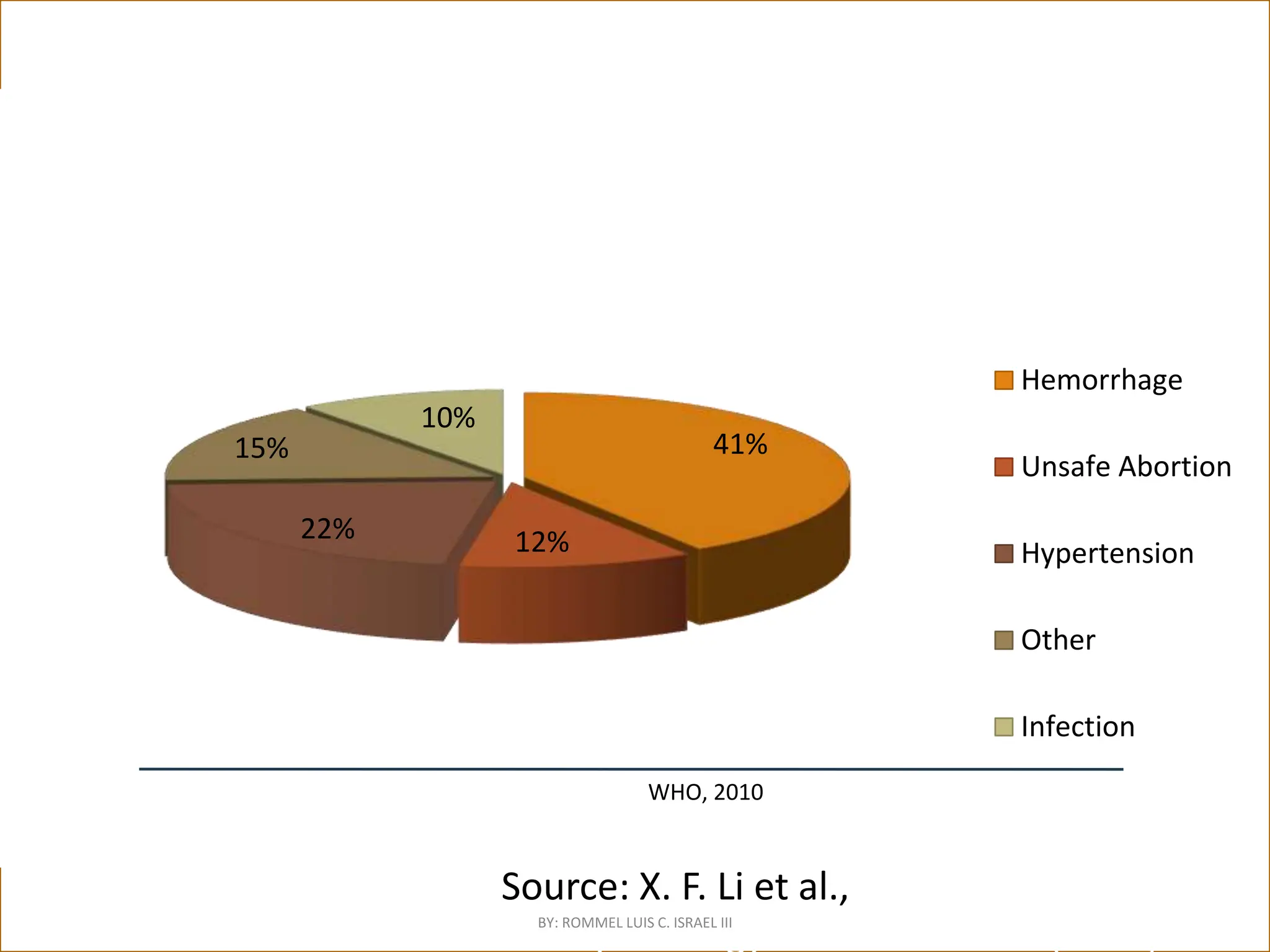
Source: X. F. Li et al., International Joumal of
Gynecology & Obstetrics 54 (1996): 1-10
Percent
of
maternal
deaths
in
developing
countries
41%
12%
22%
15%
10%
Hemorrhage
Unsafe Abortion
Hypertension
Other
Infection
WHO, 2010
BY: ROMMEL LUIS C. ISRAEL III
ANTENATAL
CARE
At lease 4antenatal visits
with a skilled health
provider
•To detect diseases which
may complicate pregnancy
•To educate women on
danger and emergency
signs & symptoms
•To prepare the woman and
her family for childbirth
BY: ROMMEL LUIS C. ISRAEL III 6
7.
To detect diseaseswhich may complicate
pregnancy
Screen
Anemia
Pre-eclampsia
Diabetes Mellitus
Syphilis
Detect
PROM
Preterm labor
◦ Ferrous and folic acid
supplementation
◦ Tetanus toxoid immunization
◦ Corticosteroids for preterm
labor
Treat
◦ Ferrous sulfate for anemia
◦ Antihypertensive meds and
Magnesium sulfate for SEVERE pre-
eclampsia
◦ REFER
• Prevent
BY: ROMMEL LUIS C. ISRAEL III 7
8.
Antenatal Corticosteroids
Administer ANTENATALSTEROIDS to
all patients who are at risk for preterm
delivery
◦with preterm labor between 24-34 weeks
AOG
◦or with any of the following prior to term:
◦ Antepartal hemorrhage/bleeding
◦ Hypertension
◦ (preterm) Pre-labor rupture of membranes
BY: ROMMEL LUIS C. ISRAEL III 8
9.
Antenatal Steroids
Overall reductionin neonatal death
Reduction in RDS
Reduction in cerebroventricular
hemorrhage
Reduction in sepsis in the first 48 hours of
life
Roberts D, Dalziel SR. Cochrane Database of
Systematic Reviews 2006, Issue 3.
Betamethasone 12 mg IM q 24 hrs x 2 doses OR
DEXAMETHASONE 6 mg IM q 12 x 4 doses
BY: ROMMEL LUIS C. ISRAEL III 9
10.
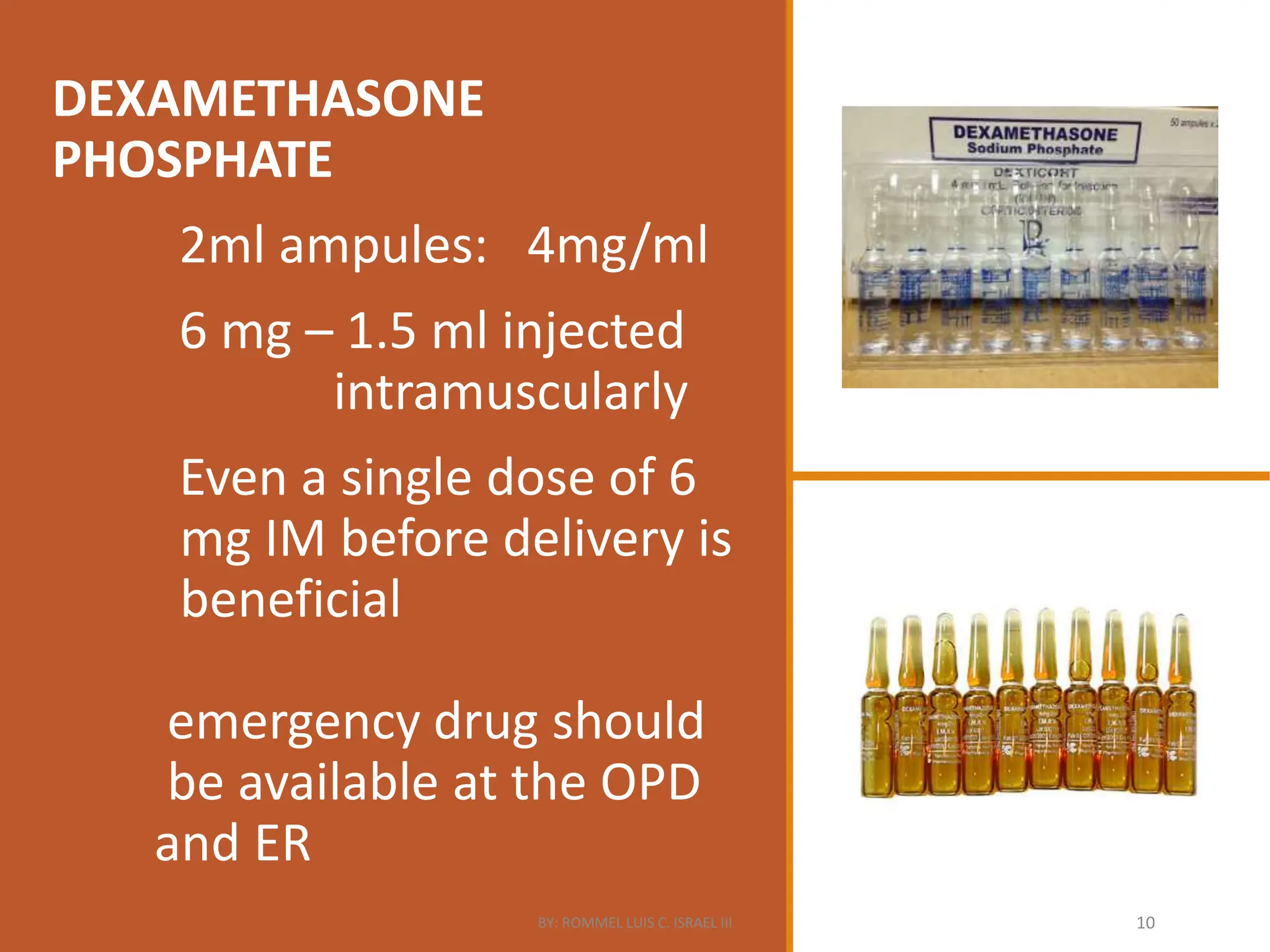
DEXAMETHASONE
PHOSPHATE
2ml ampules: 4mg/ml
6mg – 1.5 ml injected
intramuscularly
Even a single dose of 6
mg IM before delivery is
beneficial
emergency drug should
be available at the OPD
and ER
BY: ROMMEL LUIS C. ISRAEL III 10
11.
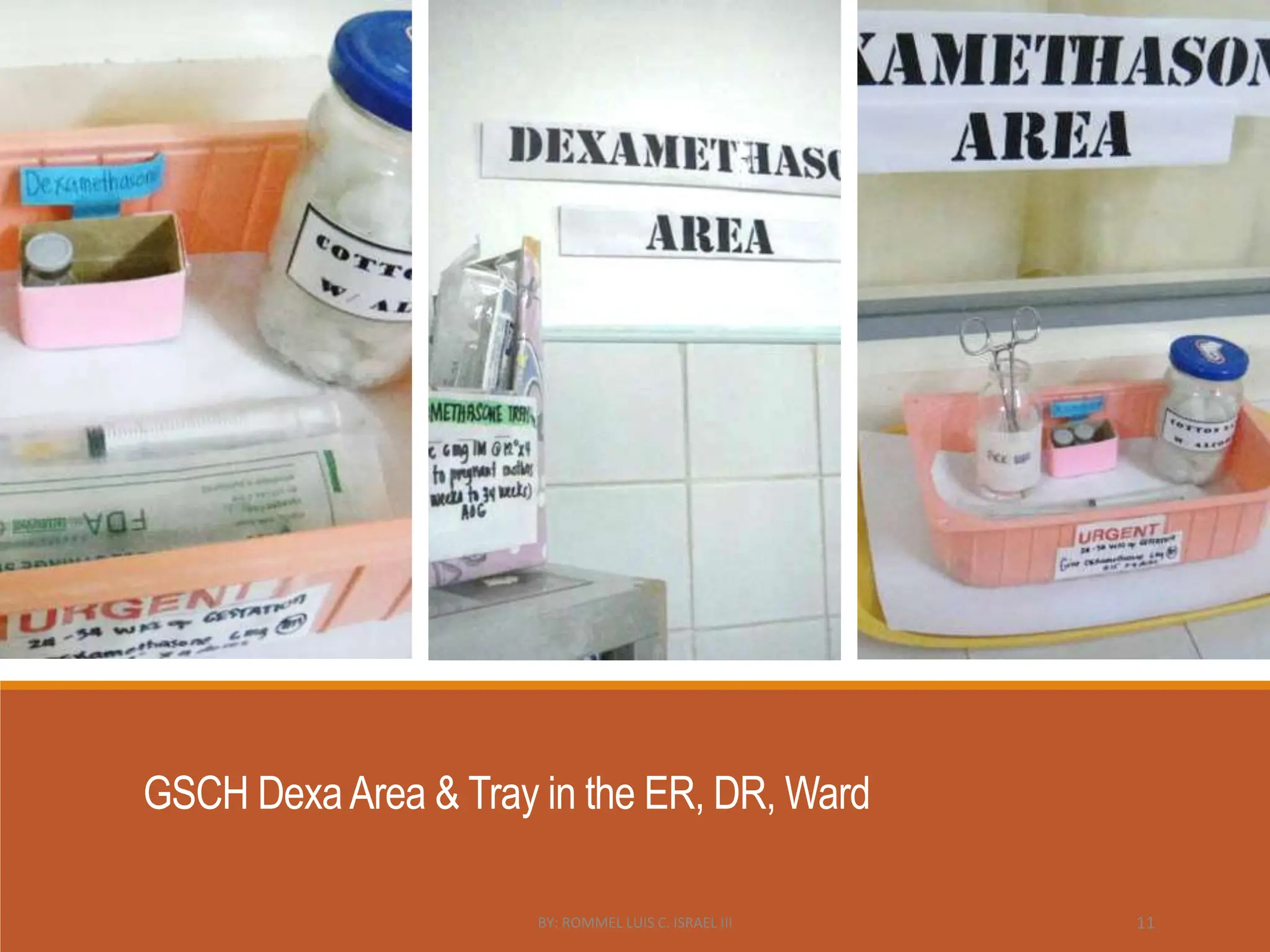
GSCH DexaArea &Tray in the ER, DR, Ward
BY: ROMMEL LUIS C. ISRAEL III 11
12.
DANGER SIGNS andSYMPTOMS
Vaginal bleeding
Headache
Blurring of vision
Abdominal Pain
Severe difficulty breathing
Dangerous fever (T°>38, weak)
Burning on urination
Educate women on
BY: ROMMEL LUIS C. ISRAEL III 12
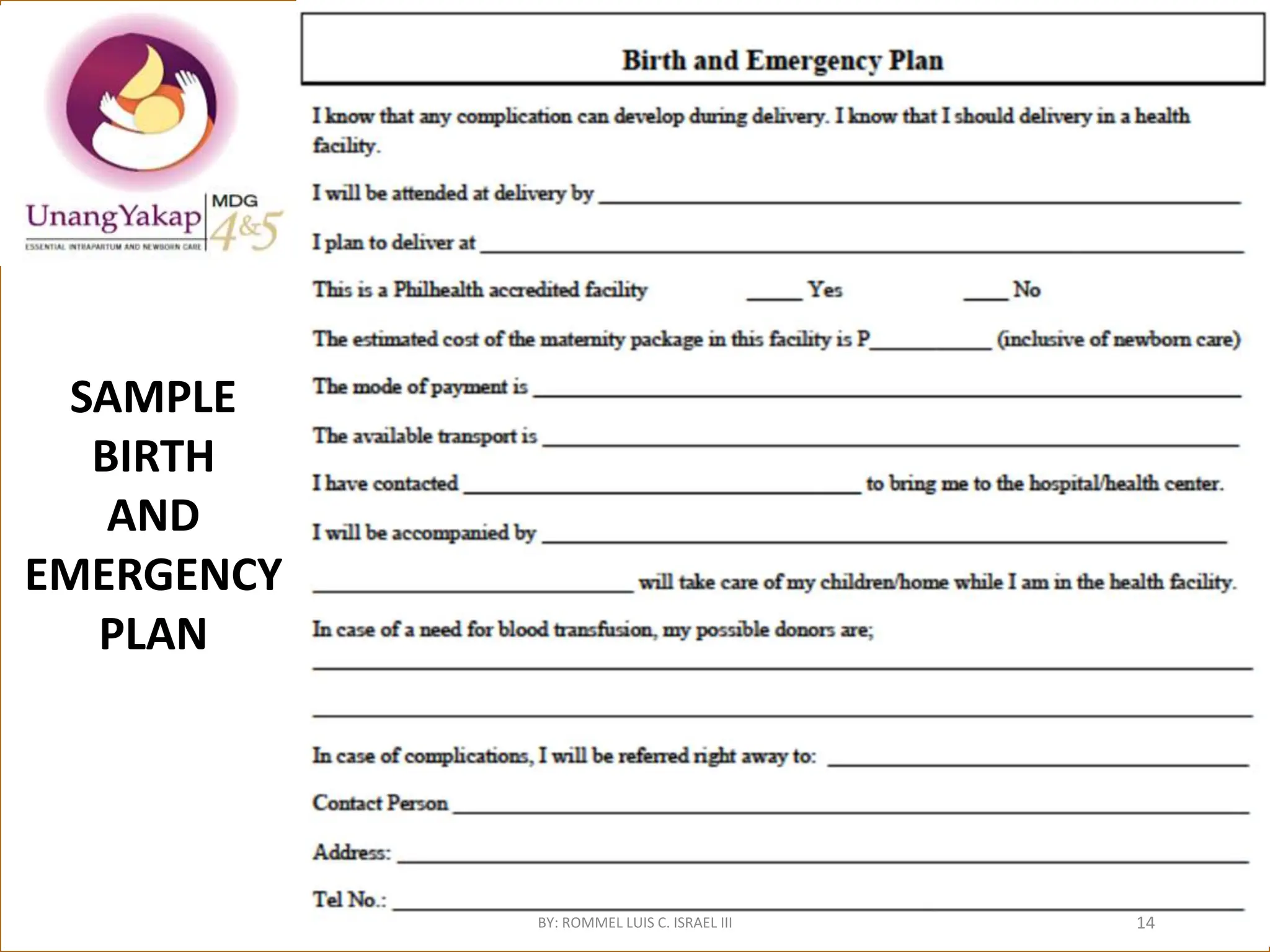
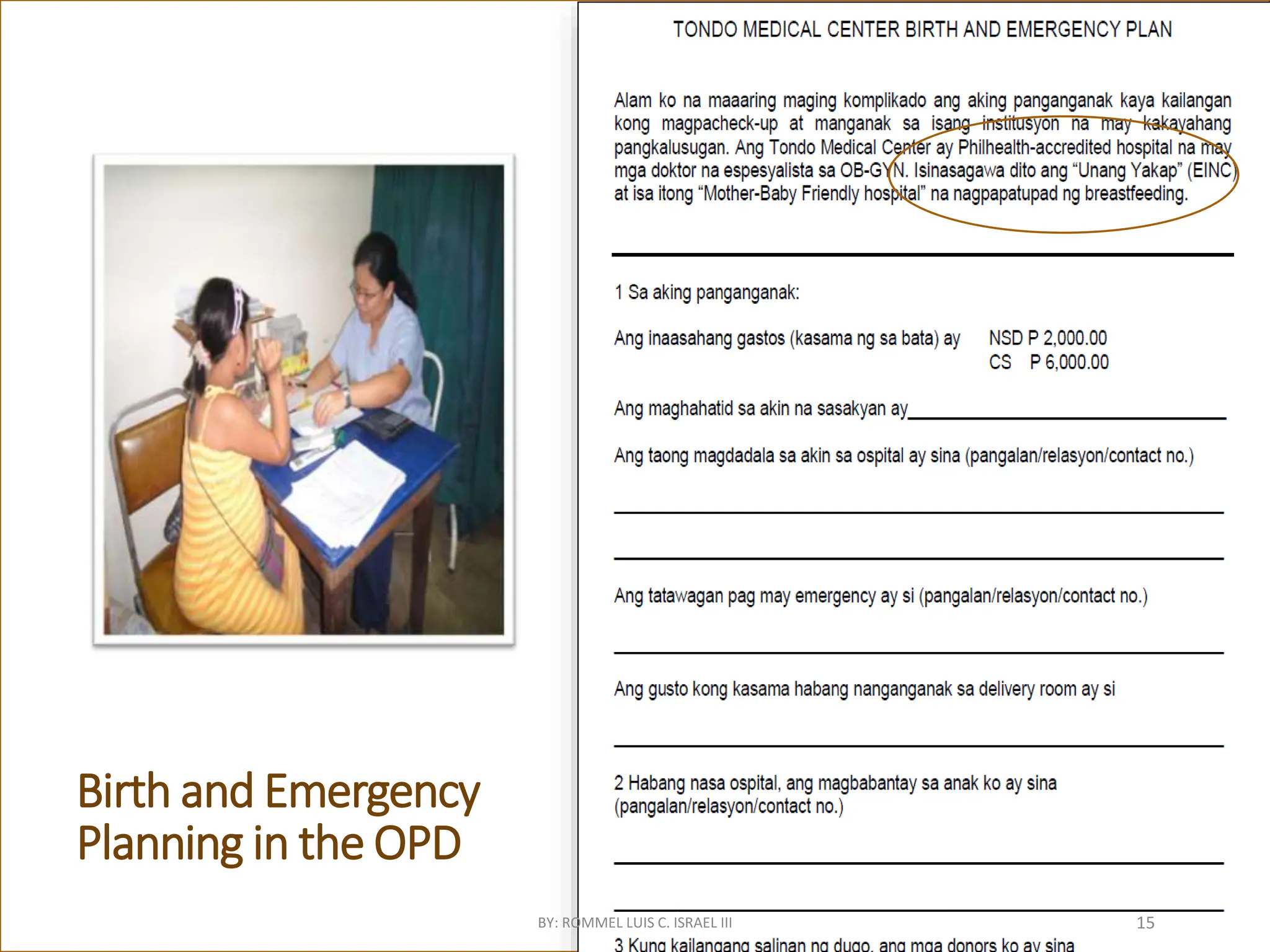
13.
Prepare the
woman and
herfamily for
childbirth
Counsel on
◦ Proper nutrition and self care
during pregnancy
◦ Breastfeeding and family planning
BIRTH PLAN
◦ Where she will deliver;
transportation
◦ Who will assist her delivery
◦ What to expect during labor and
delivery
◦ What to prepare, estimated cost of
delivery
◦ Possible blood donors; where will
she be referred in case of
emergency
BY: ROMMEL LUIS C. ISRAEL III 13
Recommended Practices DuringLabor
•Active phase labor:
– 2-3 contractions in 10 minutes
– Cervix is 4 cm dilated
1. Admission to
labor when the
parturient is
already in the
active phase.
BY: ROMMEL LUIS C. ISRAEL III 18
19.
Recommended Practices DuringLabor:
Admit when the parturient is already in ACTIVE
LABOR
No difference in Apgar score
•↓need for Cesarean Section by 82%
No difference in need for labor
augmentation
Rahnama, P., et.al., 2006: prospective
cohort study on 810 low risk nulliparas (474
in latent phase; 336 in active phase )
BY: ROMMEL LUIS C. ISRAEL III 19
20.
Recommended Practices
During Labor
1.Admission to
labor when the
parturient is
already in the
active phase.
2. Continuous
maternal
support
BY: ROMMEL LUIS C. ISRAEL III 20
21.
Continuous maternal support
•↓Needfor pain relief by 10%
•Duration of labor SHORTER by half an hour
•↑spontaneous vaginal delivery by 8%
•↓ Instrumental vaginal delivery 10%
•5 minute Apgar < 7 ↓ by 30%
Source of evidence: Cochrane review (21 trials, 15,061
women) comparing one-to-one intrapartum support
given by variety of providers (nurses, midwives, doulas,
partner, female relative, friend) versus usual care
(Hodnett, E.D., et.al., 2011)
BY: ROMMEL LUIS C. ISRAEL III 21
22.
Having a LABOR
COMPANIONcan result in:
• Less use of pain relief drugs →
Increased alertness of baby
• Baby less stressed , uses less energy
– Reduced risk of infant hypothermia
– Reduced risk of hypoglycemia
• Early and frequent breastfeeding
• Easier bonding with the baby
BY: ROMMEL LUIS C. ISRAEL III 22
23.
Recommended
Practices During
Labor
1.Admission tolabor
when the parturient is
already in the active
phase.
2.Continuous maternal
support
3.Upright position during
first stage of labor
BY: ROMMEL LUIS C. ISRAEL III 23
24.
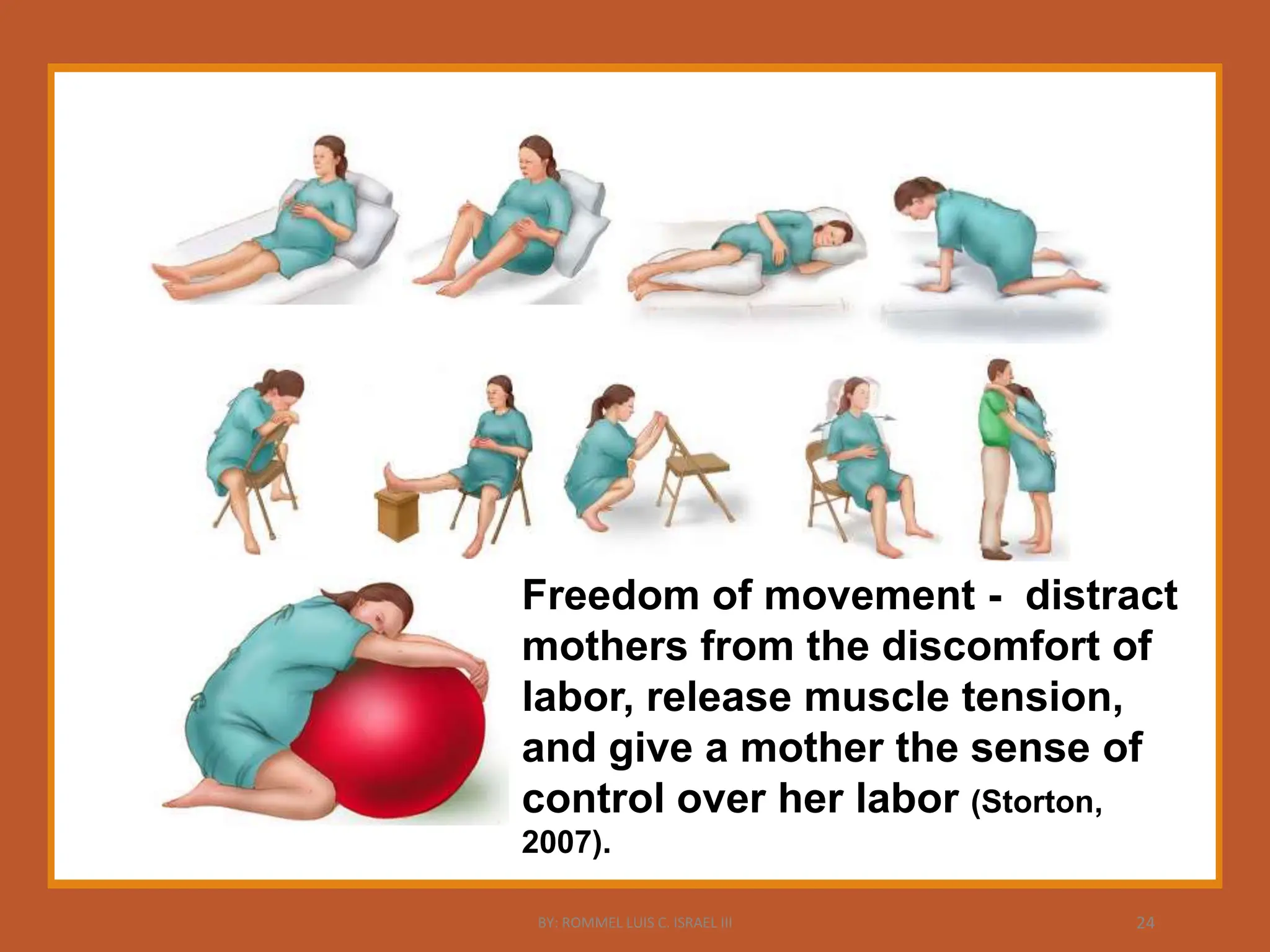
Freedom of movement- distract
mothers from the discomfort of
labor, release muscle tension,
and give a mother the sense of
control over her labor (Storton,
2007).
BY: ROMMEL LUIS C. ISRAEL III 24
25.
UPRIGHT POSITION
DURING LABOR
Firststage of labor shorter by
about 1 hour
Need for epidural analgesia ↓ by
17%
No difference in rates of SVD , CS,
and Apgar score < 7 at 5 minutes
Source of Evidence: Cochrane review (21 studies involving 3,706 women) comparing upright
versus recumbent position (Lawrence, A., et.al., 2009)
BY: ROMMEL LUIS C. ISRAEL III 25
26.
Restricting practices limita
mother’s freedom to move
and/or her position of
choice.
1. IV lines*
2. fetal monitoring
3. labor stimulating
medications that require
monitoring of uterine activity,
4. small labor rooms,
5. epidural placement
6. absence of support persons
to “be with” the intrapartum
client
BY: ROMMEL LUIS C. ISRAEL III 26
27.
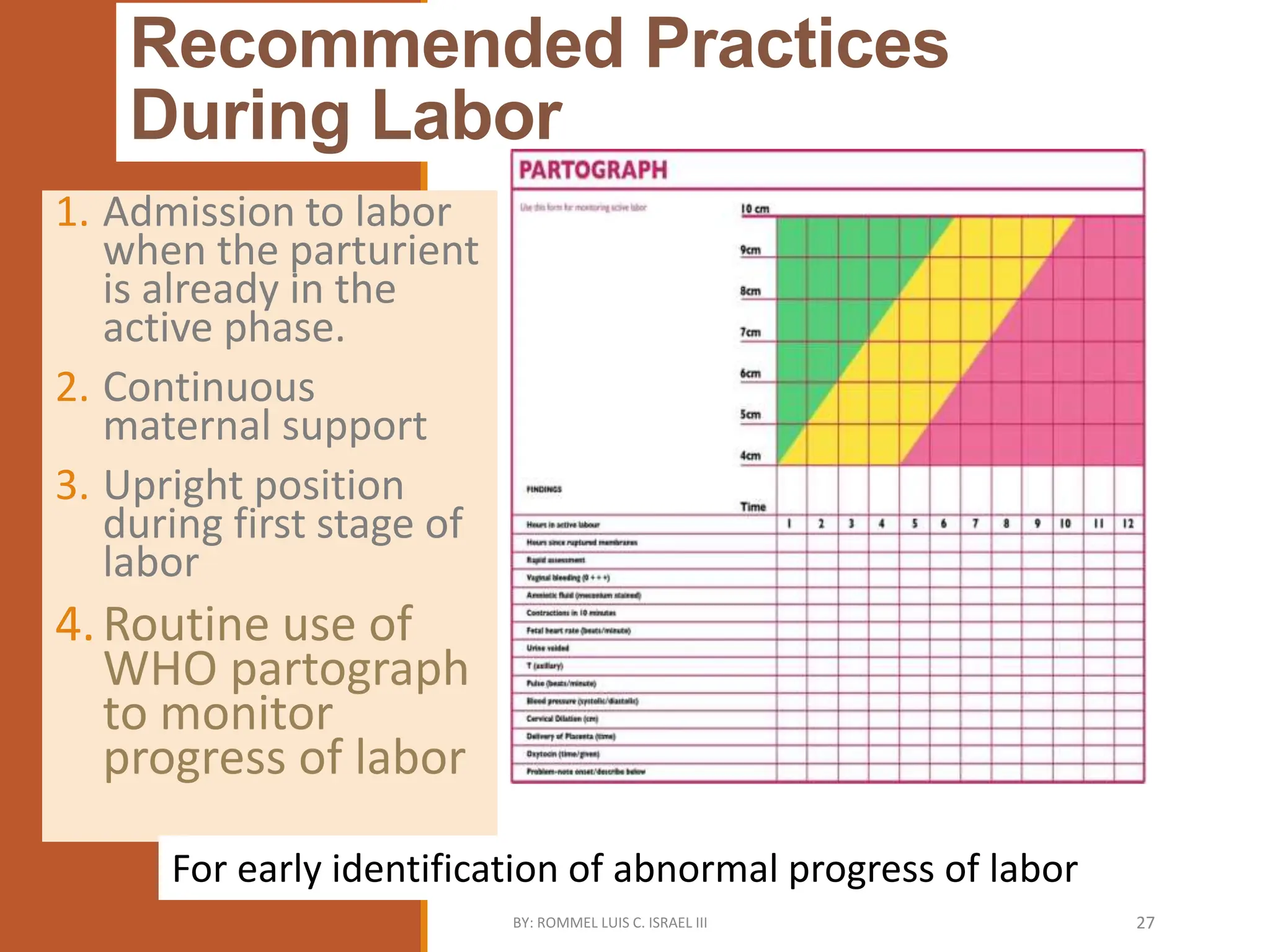
Recommended Practices
During Labor
1.Admission to labor
when the parturient
is already in the
active phase.
2. Continuous
maternal support
3. Upright position
during first stage of
labor
4.Routine use of
WHO partograph
to monitor
progress of labor
For early identification of abnormal progress of labor
BY: ROMMEL LUIS C. ISRAEL III 27
28.
Recommended Practices DuringLabor
No difference in
endometritis
UTI lower by 34%
An observational study on 161,077
women (with or w/o PPROM) who had <
5 exams (Ayzac, L., et.al., 2008)
↓ Chorioamnionitis by 72%
↓ Neonatal sepsis by 61%
1 RCT on 5,018 women with PROM
comparing < 3 exams vs 3 exams
(Seaward, P.G., et.al., 1998)
1. Admission to labor
when the parturient
is already in the
active phase.
2. Continuous maternal
support
3. Upright position
during first stage of
labor
4. Routine use of WHO
partograph to
monitor progress of
labor
5. Limit total number of
IE to 5 or less.
BY: ROMMEL LUIS C. ISRAEL III 28
Interventions that areNOT
recommended during labor
No difference in rates
of maternal fever,
perineal wound
infection, and perineal
wound dehiscence
No neonatal infection
was observed
1.Routine
perineal
shaving
on
admission
for labor
and
delivery.
Evidence: Cochrane review (3 trials) comparing it with
no shaving (Basevi, V. and Lavender, T., 2000
updated 2008)
BY: ROMMEL LUIS C. ISRAEL III 30
31.
Interventions that areNOT
recommended during labor
Fecal soiling during delivery reduced
by 64%
No difference in maternal puerperal
infection, episiotomy dehiscence,
neonatal infection, and neonatal
pneumonia
1.Routine
perineal
shaving on
admission
for labor
and
delivery.
2.Routine
enema
during the
first stage
of labor.
Source of Evidence: Cochrane review (4 trials)
comparing it with no enema (Reveiz, L., et.al.
2007 updated 2010)
BY: ROMMEL LUIS C. ISRAEL III 31
32.
Practices that areNOT
recommended during labor
No difference in
chorioamnionitis,
postpartum endometritis,
perinatal mortality, neonatal
sepsis
No side effects reported
1. Routine
perineal
shaving on
admission
for labor and
delivery.
2. Routine
enema
during the
first stage of
labor.
3. Routine
vaginal
douching.
Source of Evidence: Cochrane review
(3 trials that used different concentrations
and volumes of Chlorhexidine) comparing it
with sterile saline (Lumbiganon, P., et.al.,
2004 updated 2009)
BY: ROMMEL LUIS C. ISRAEL III 32
33.
Practices that areNOT
recommended during labor
↓Risk of dysfunctional labor
by 25%
No difference in duration of
labor, CS rate, cord prolapse,
maternal infection and
Apgar score < 7 at 5
minutes
1. Routine perineal
shaving on
admission for
labor and
delivery.
2. Routine enema
during the first
stage of labor.
3. Routine vaginal
douching.
4. Routine
amniotomy to
shorten
spontaneous
labor
Source of Evidence: Cochrane review -14 trials
involving 4,893 women. (Smyth, R.M.D., et.al.,
2007 updated 2010)
BY: ROMMEL LUIS C. ISRAEL III 33
34.
Oxytocin
Augmentation
Should only beused to augment
labor in facilities where there is
immediate access to caesarean
section should the need arise.
Use of any IM oxytocin before
the birth of the infant is generally
regarded as dangerous because
the dosage cannot be adapted to
the level of uterine activity.
BY: ROMMEL LUIS C. ISRAEL III
35.
Routine IVF
ADVANTAGE
to haveready
access for
emergency
medications
to maintain
maternal
hydration
DISADVANTAGE
Interferes with the natural
birthing process
restricts woman’s freedom
to move
IVF not as effective as
allowing food and fluids in
labor to treat/prevent
dehydration, ketosis or
electrolyte imbalance
POGS CPG on NORMAL LABOR AND DELIVERY, 2009
BY: ROMMEL LUIS C. ISRAEL III 35
36.
Routine IVF
No studyfound showing that
having an IV in place improves
outcome
Even the prophylactic insertion of
an IV line should be considered
unnecessary intervention.
Philippine Ob-Gyn Society CPG on
Normal Labor and Delivery, 2009
BY: ROMMEL LUIS C. ISRAEL III 36
37.
Routine NPO DuringLabor
Possible risk of aspirating gastric contents with the
administration of anesthesia
One study evaluated the probable risk of maternal aspiration
mortality, which is approximately 7 in 10 million births.
No evidence of improved outcomes for mother or newborn.
Use of epidural anesthesia for intrapartum anesthesia in an
otherwise normal labor should not preclude oral intake.
Sleutel, M., and Golden, S., 1999
POGS CPG on Normal Labor and Delivery, 2009
BY: ROMMEL LUIS C. ISRAEL III 37
38.
Routine NPO DuringLabor
For the normal, low risk birth, there is no need for restriction
of food except where intervention is anticipated.
A diet of easy to digest foods and fluids during labor is
recommended.
Isotonic calorific drinks consumed during labor reduce the
incidence of maternal ketosis without increasing gastric
volumes.
Singata M, Tranmer J, Gyte GML. Restricting oral fluid and food intake during labour.
Cochrane Database of Systematic Reviews 2010, Issue 1.
POGS CPG ON NORMAL LABOR AND DELIVERY, 2009
WHO Care in Normal Birth, 1996
BY: ROMMEL LUIS C. ISRAEL III 38
39.
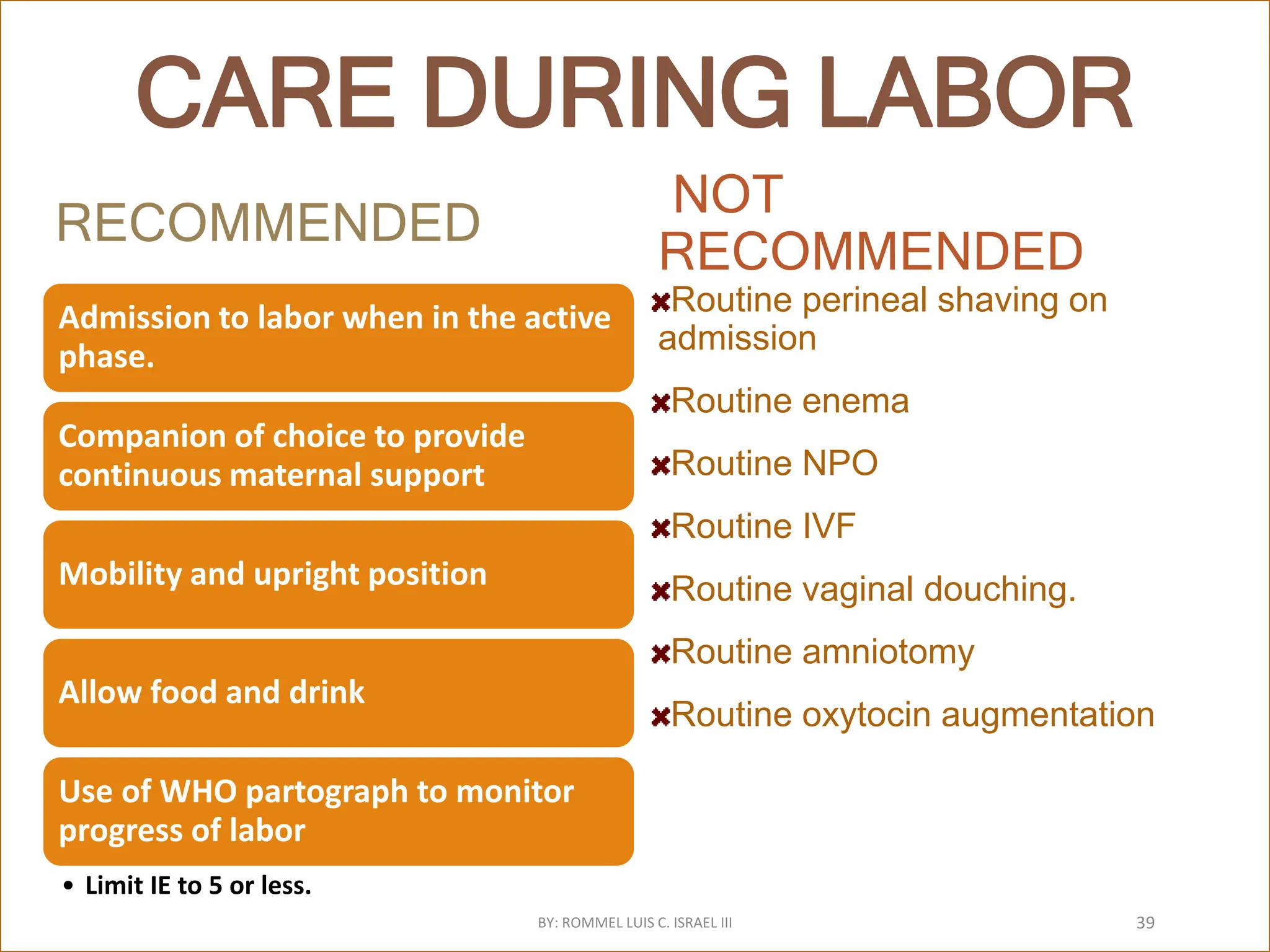
CARE DURING LABOR
RECOMMENDED
Admissionto labor when in the active
phase.
Companion of choice to provide
continuous maternal support
Mobility and upright position
Allow food and drink
Use of WHO partograph to monitor
progress of labor
• Limit IE to 5 or less.
NOT
RECOMMENDED
Routine perineal shaving on
admission
Routine enema
Routine NPO
Routine IVF
Routine vaginal douching.
Routine amniotomy
Routine oxytocin augmentation
BY: ROMMEL LUIS C. ISRAEL III 39
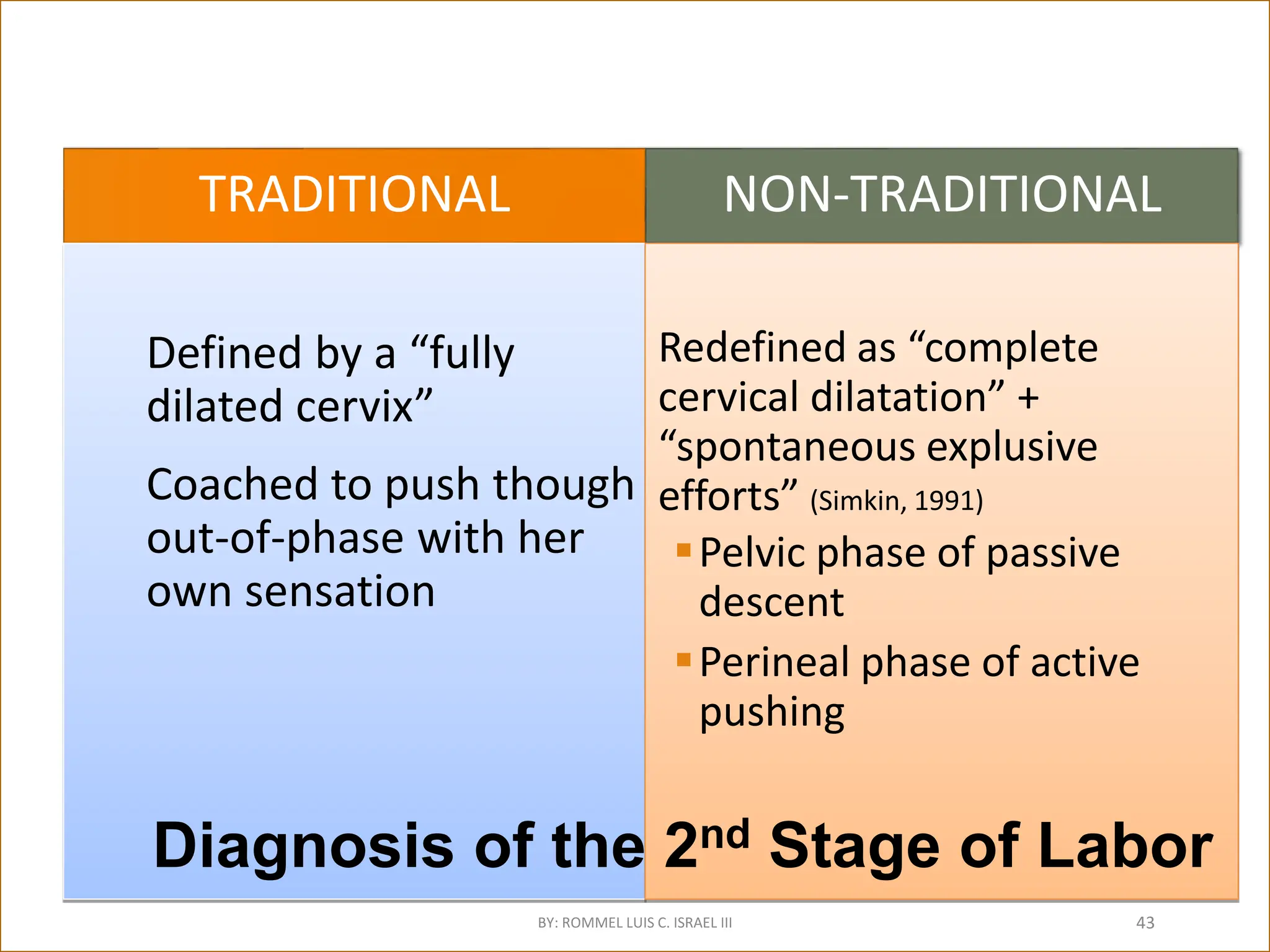
TRADITIONAL
Defined by a“fully
dilated cervix”
Coached to push though
out-of-phase with her
own sensation
NON-TRADITIONAL
Redefined as “complete
cervical dilatation” +
“spontaneous explusive
efforts” (Simkin, 1991)
Pelvic phase of passive
descent
Perineal phase of active
pushing
Diagnosis of the 2nd Stage of Labor
BY: ROMMEL LUIS C. ISRAEL III 43
Management of the2nd Stage of Labor
TRADITIONAL
DIRECTED PUSHING
Valsalva pushing
Venous Return
Perfusion to Uterus, Placenta & Fetus
FHR Changes
Fetal hypoxia & acidosis
Roberts,1996; Simkin, 2000;Roberts,1987 as cited in Roberts, Joyce,Journal of Midwifery
and Women’s Health.Vol. 47,No.1 Jan/Feb 2002
NON-TRADITIONAL
INVOLUNTARY BEARING DOWN
Exhalation pushing
Let air out
Parturient-directed
Physiologic: force of bearing down efforts
increases as fetal descent occurs
Avoids hypoxia and acidosis
Nikodem,VC. Beaaring down Methods during second stage labour (Cochrane Review) In:
The Cochrane Library, Issue 2, 2001 as cited by Roberts, 2002
BY: ROMMEL LUIS C. ISRAEL III 45
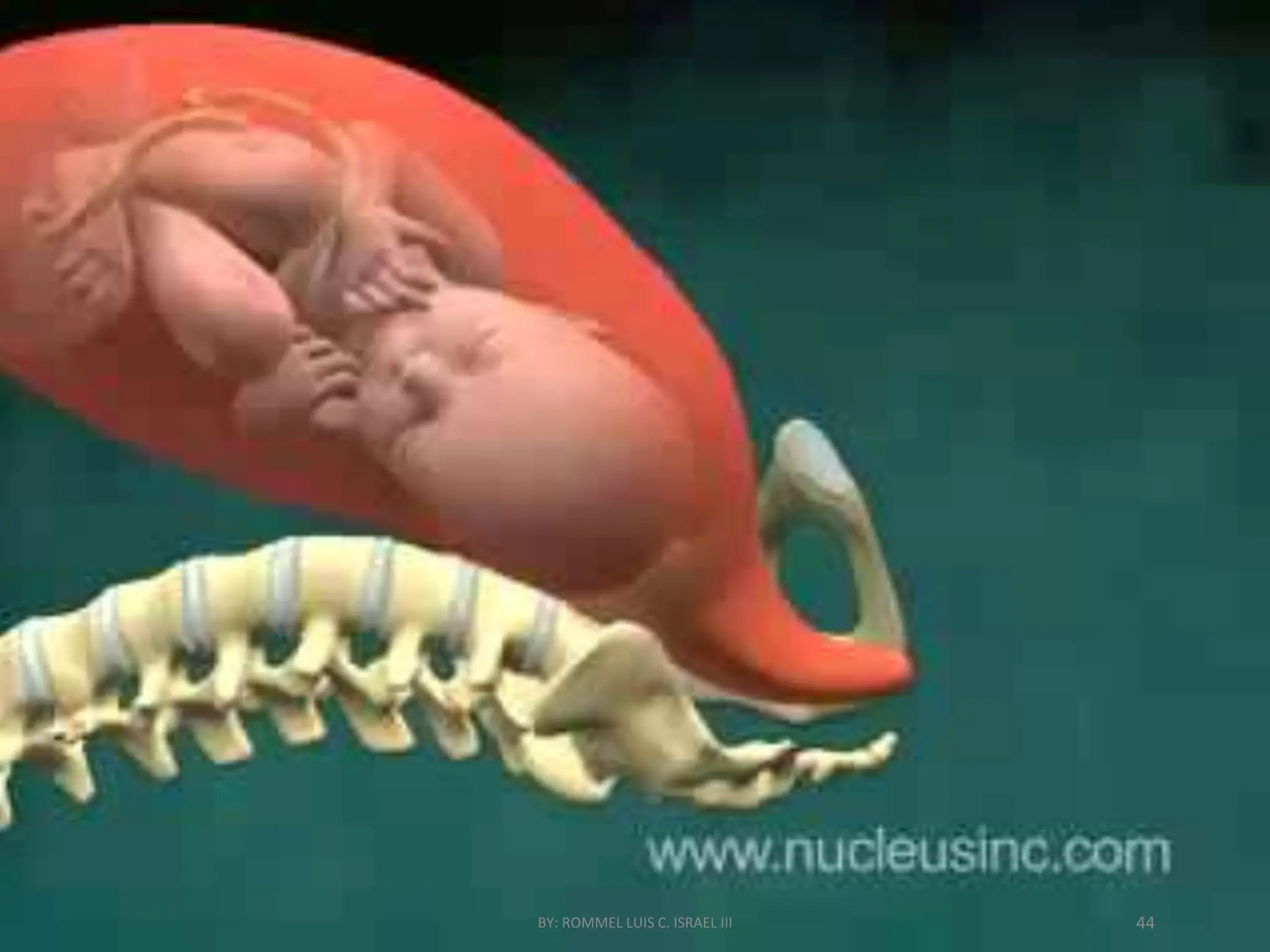
46.
UPRIGHT
position
during
delivery
More efficientuterine
contractions
Improved fetal alignment
Larger anterior-posterior and
transverse diameters of pelvic
outlet enhances fetal
movement through the maternal
pelvis in descent for birth
Faster delivery
Leads to less interventions : less
episiotomies.
Shilling, Romano, & DiFranco, 2007
BY: ROMMEL LUIS C. ISRAEL III 46
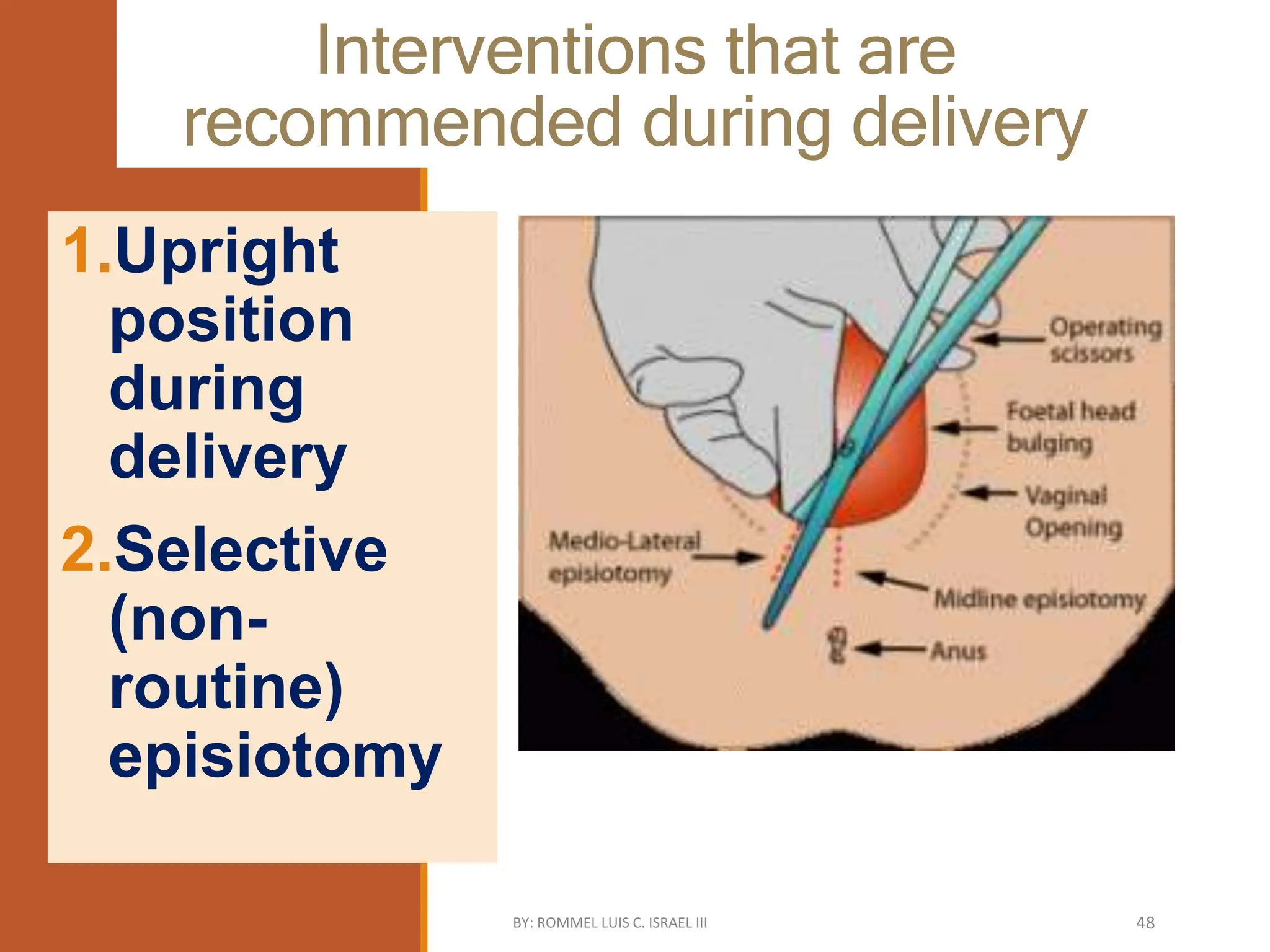
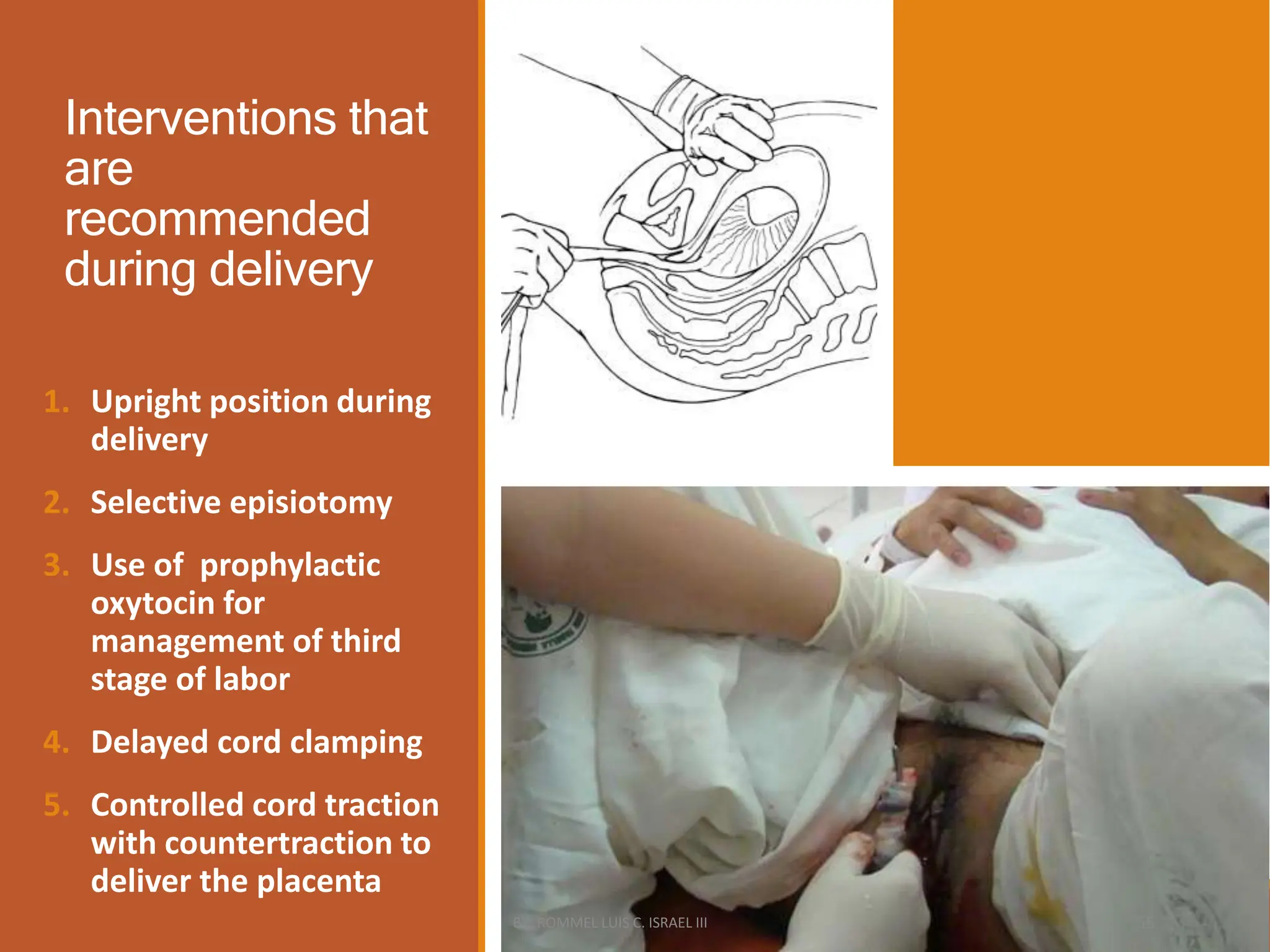
Interventions that are
recommendedduring delivery
1.Upright
position
during
delivery
2.Selective
(non-
routine)
episiotomy
BY: ROMMEL LUIS C. ISRAEL III 48
49.
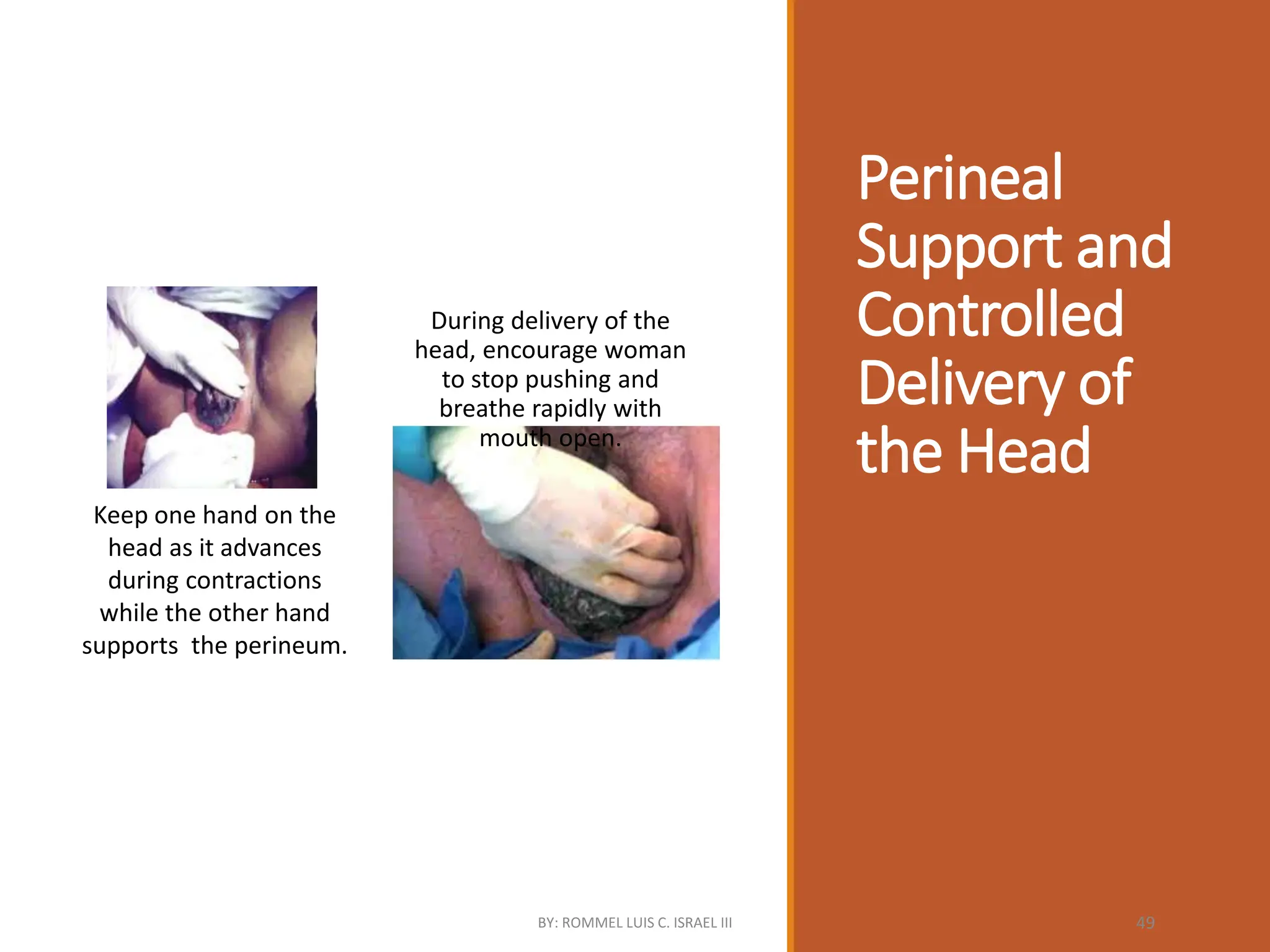
Perineal
Support and
Controlled
Delivery of
theHead
Keep one hand on the
head as it advances
during contractions
while the other hand
supports the perineum.
During delivery of the
head, encourage woman
to stop pushing and
breathe rapidly with
mouth open.
BY: ROMMEL LUIS C. ISRAEL III 49
50.
Non-Routine Episiotomy
↑Anterior perinealtrauma by 84%
↓ Posterior perineal trauma by 12%
↓ 2nd-4th degree tears by 33%
↓ Need for suturing by 29%
No difference in infection rate
Source of Evidence: Cochrane review (8 trials) that include both primis and multis and
used median or mediolateral episiotomy (Carroli, G., and Mignini, L., 2009)
BY: ROMMEL LUIS C. ISRAEL III 50
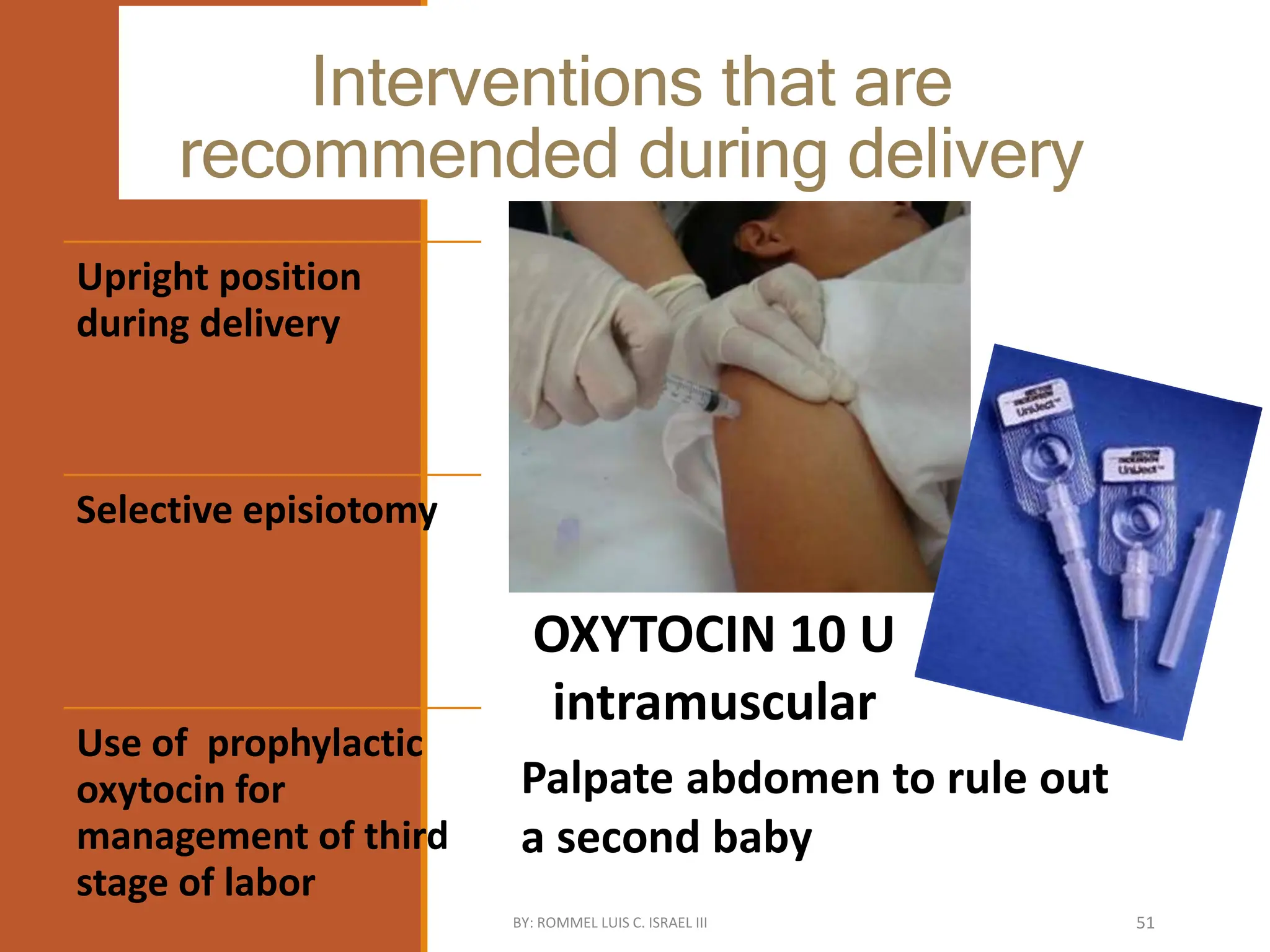
51.
Interventions that are
recommendedduring delivery
OXYTOCIN 10 U
intramuscular
Palpate abdomen to rule out
a second baby
Upright position
during delivery
Selective episiotomy
Use of prophylactic
oxytocin for
management of third
stage of labor
BY: ROMMEL LUIS C. ISRAEL III 51
52.
Prophylactic
OXYTOCIN
for the 3rd
stageof
labor
Postpartum blood loss ≥
500 ml reduced by 39%
Need for additional
uterotonic reduced by 47%
No difference in need for
maternal blood
transfusion, need for
manual removal of
placenta, and duration of
third stage
Source of Evidence: Cochrane review (4 trials on 2,213 women) using
varied doses, route, and timing of administration of oxytocin (Cotter,
A.M., et.al., 2002 updated 2004)
BY: ROMMEL LUIS C. ISRAEL III 52
53.
Interventions that are
recommendedduring delivery
Early clamping : <1 min after birth
Delayed (properly timed) :1-3
minutes after birth or when
pulsations stop
1. Upright position
during delivery
2. Selective
episiotomy
3. Use of
prophylactic
oxytocin for mgt
of 3rd stage of
labor
4. Delayed cord
clamping
BY: ROMMEL LUIS C. ISRAEL III 53
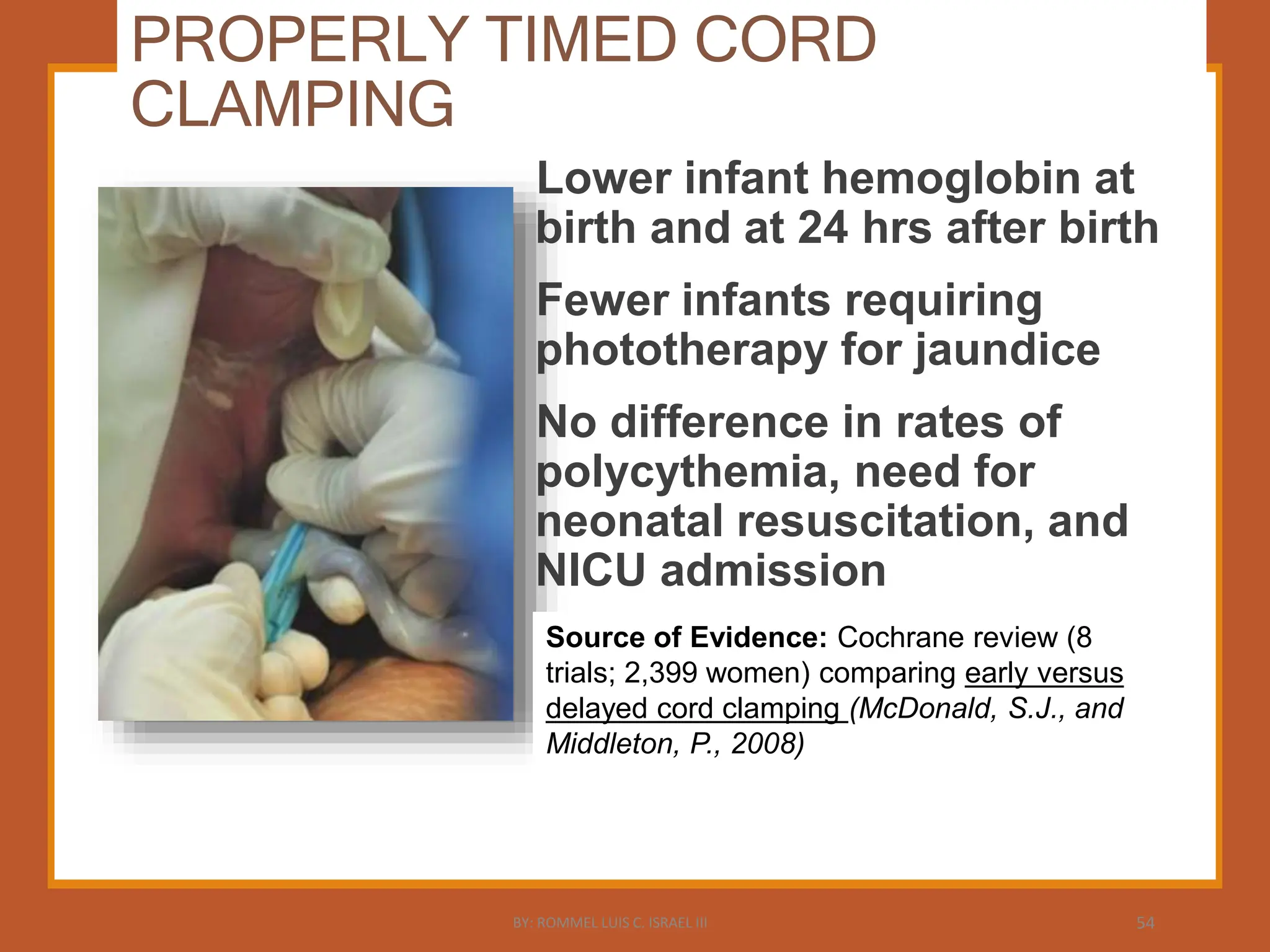
54.
PROPERLY TIMED CORD
CLAMPING
Lowerinfant hemoglobin at
birth and at 24 hrs after birth
Fewer infants requiring
phototherapy for jaundice
No difference in rates of
polycythemia, need for
neonatal resuscitation, and
NICU admission
Source of Evidence: Cochrane review (8
trials; 2,399 women) comparing early versus
delayed cord clamping (McDonald, S.J., and
Middleton, P., 2008)
BY: ROMMEL LUIS C. ISRAEL III 54
55.
Interventions that
are
recommended
during delivery
1.Upright position during
delivery
2. Selective episiotomy
3. Use of prophylactic
oxytocin for
management of third
stage of labor
4. Delayed cord clamping
5. Controlled cord traction
with countertraction to
deliver the placenta
BY: ROMMEL LUIS C. ISRAEL III 55
56.
Controlled Cord Traction
↓Postpartumblood loss >500ml by 7%
↓Postpartum blood loss >100ml by
24%
No difference in rates of maternal
mortality or serious morbidity and need
for additional uterotonics.
Source of Evidence: Pooled analysis of 2 RCTs (23000 subjects) comparing it
with the “hands off” approach. (Althabe, F et al, 2009; Gulmezoglu AM et
al, 2012)
BY: ROMMEL LUIS C. ISRAEL III 56
57.
Interventions that arerecommended
during delivery
1. Upright position
during delivery
2. Selective
episiotomy
3. Use of prophylactic
oxytocin
4. Delayed cord
clamping
5. Controlled cord
traction with
countertraction
6. Uterine massage
after placental
delivery
•Lower mean
blood loss
•Less need for
uterotonics
Source of evidence: Cochrane review (1 trial on 200
women who delivered vaginally and AMTSL done vs
massage. ) Hofmeyr, GJ et al 2008
BY: ROMMEL LUIS C. ISRAEL III 57
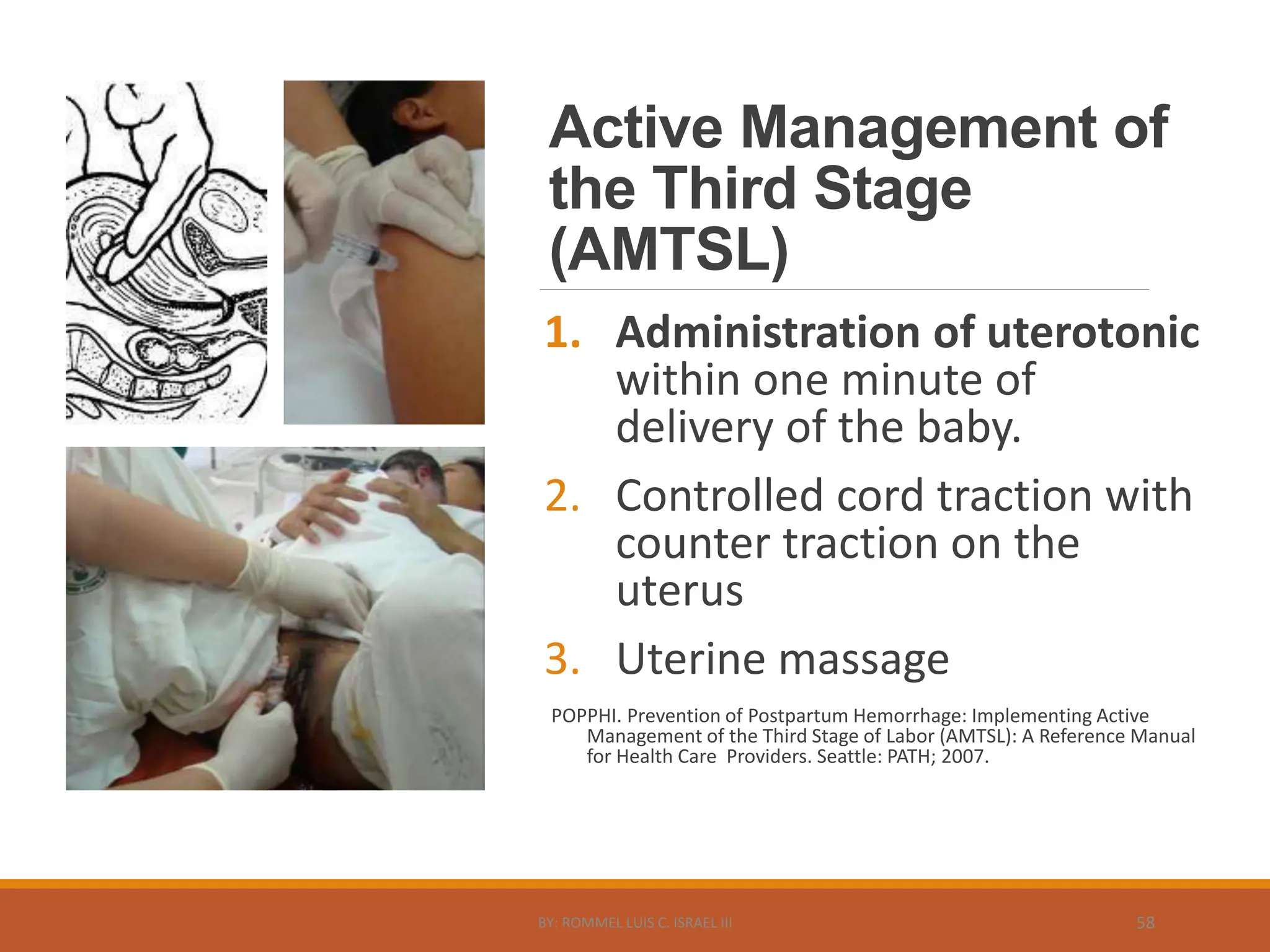
58.
Active Management of
theThird Stage
(AMTSL)
1. Administration of uterotonic
within one minute of
delivery of the baby.
2. Controlled cord traction with
counter traction on the
uterus
3. Uterine massage
POPPHI. Prevention of Postpartum Hemorrhage: Implementing Active
Management of the Third Stage of Labor (AMTSL): A Reference Manual
for Health Care Providers. Seattle: PATH; 2007.
BY: ROMMEL LUIS C. ISRAEL III 58
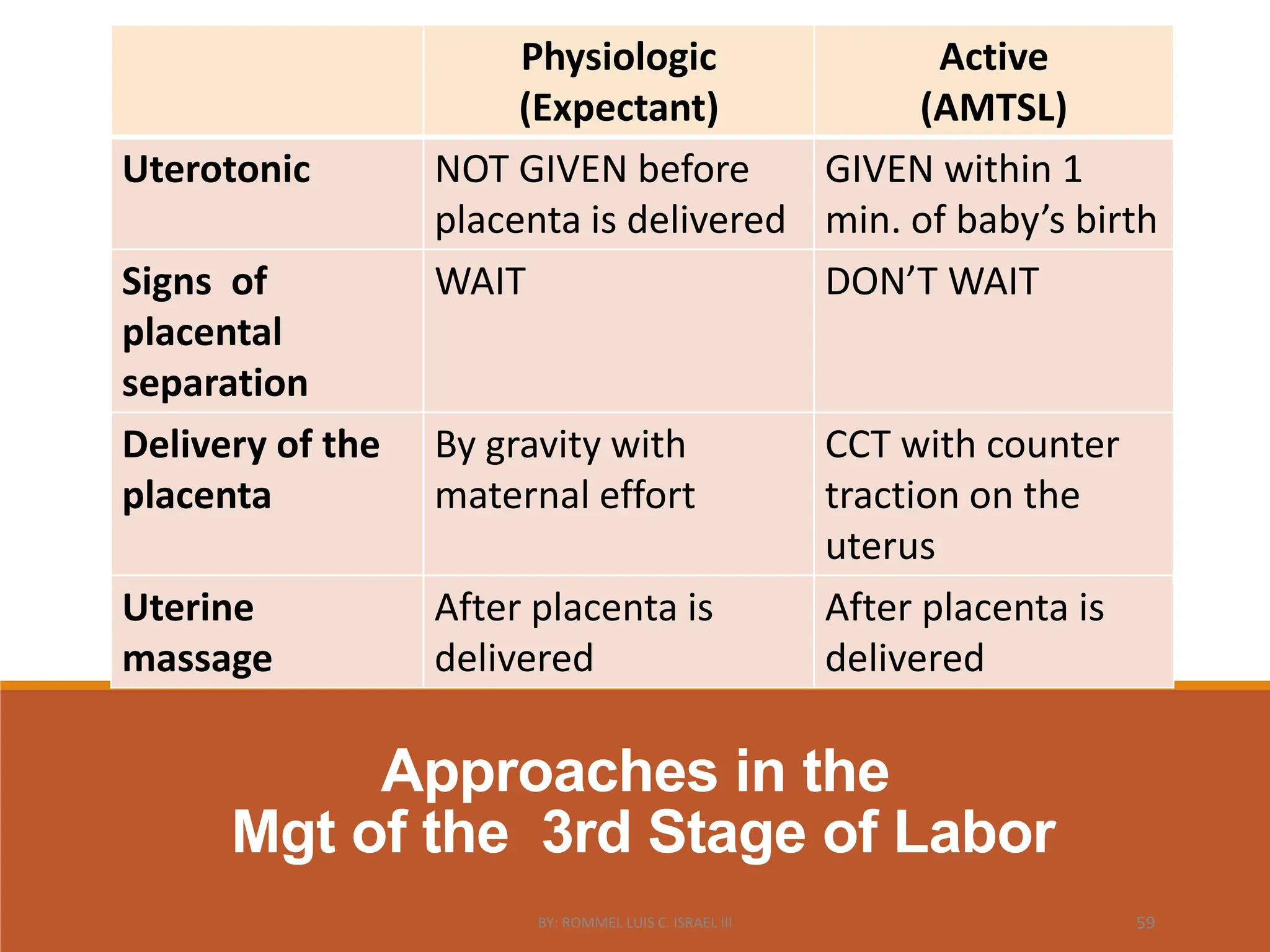
59.
Approaches in the
Mgtof the 3rd Stage of Labor
Physiologic
(Expectant)
Active
(AMTSL)
Uterotonic NOT GIVEN before
placenta is delivered
GIVEN within 1
min. of baby’s birth
Signs of
placental
separation
WAIT DON’T WAIT
Delivery of the
placenta
By gravity with
maternal effort
CCT with counter
traction on the
uterus
Uterine
massage
After placenta is
delivered
After placenta is
delivered
BY: ROMMEL LUIS C. ISRAEL III 59
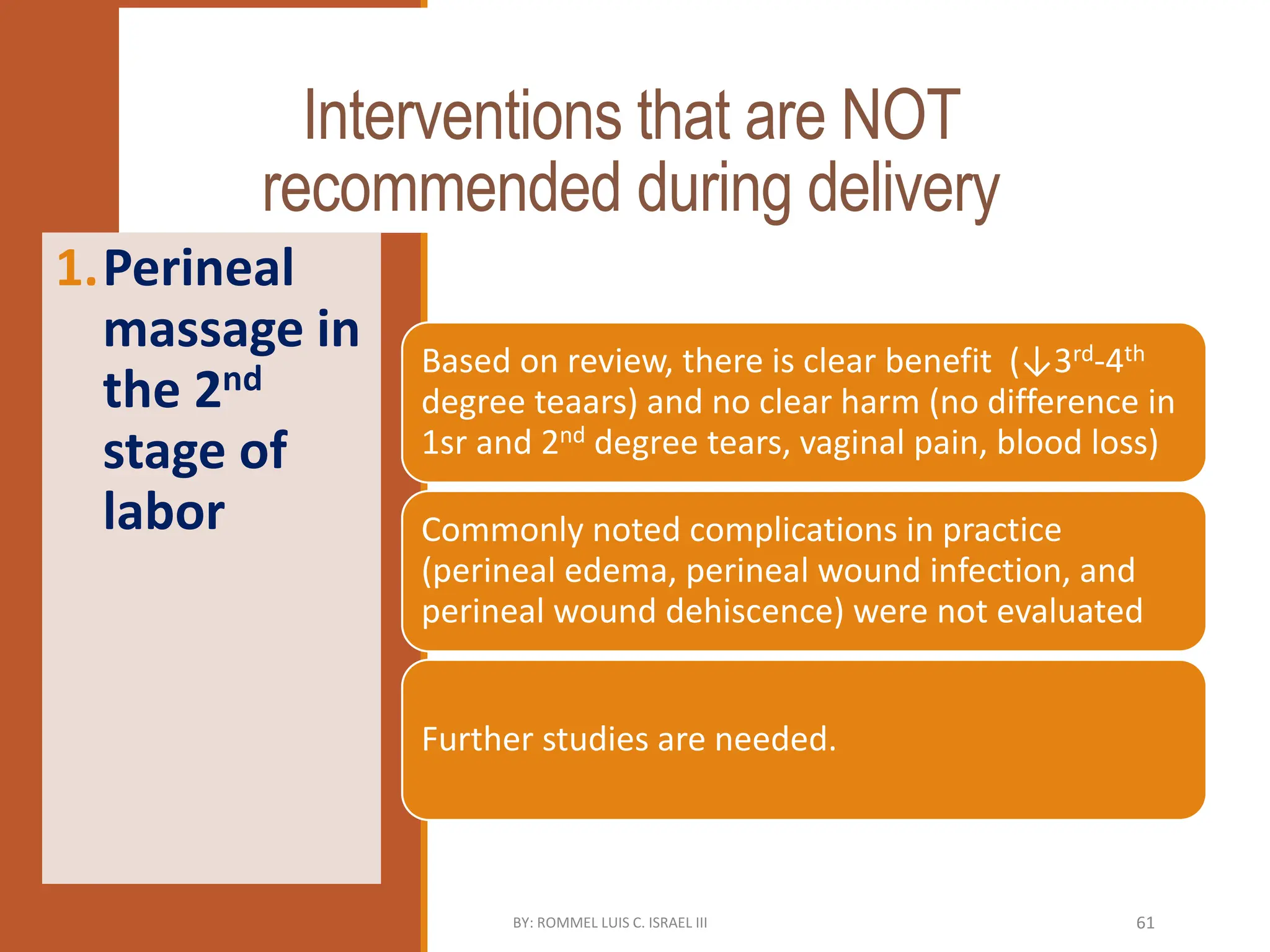
Interventions that areNOT
recommended during delivery
Based on review, there is clear benefit (↓3rd-4th
degree teaars) and no clear harm (no difference in
1sr and 2nd degree tears, vaginal pain, blood loss)
Commonly noted complications in practice
(perineal edema, perineal wound infection, and
perineal wound dehiscence) were not evaluated
Further studies are needed.
1.Perineal
massage in
the 2nd
stage of
labor
BY: ROMMEL LUIS C. ISRAEL III 61
62.
Interventions
that are NOT
recommended
duringdelivery
1. Perineal
massage in
the 2nd stage
of labor
2. Fundal
pressure
during the
second stage
of labor
BY: ROMMEL LUIS C. ISRAEL III 62
63.
Fundal
Pressure
during
2nd
stage
2nd stage longerby 29
minutes
Increased 3rd and 4th degree
perineal tears
No difference in rates of
postpartum hemorrhage,
instrumental vaginal delivery,
Apgar score < 7 at 5 minutes,
and NICU admission
Uterine rupture was not
evaluated
Source of Evidence: Pooled analysis of Cochrane review (with 1 trial
only) (Verheijen, E.C., et.al., 2009) and 2 randomized trials (Cosner,
K., 1996; Matsuo, K., et.al., 2009) with overall total of 1,229 patients
BY: ROMMEL LUIS C. ISRAEL III 63
64.
CARE DURING DELIVERY
RECOMMENDED
Uprightposition during
delivery
Selective episiotomy
Use of prophylactic
oxytocin for mgt of 3rd stage
of labor
Delayed cord clamping
Controlled cord traction with
countertraction to deliver the
placenta
Uterine massage
NOT
RECOMMENDED
Coaching the mother to
push
Perineal massage in the
2nd stage of labor
Fundal pressure during
the second stage of
labor
BY: ROMMEL LUIS C. ISRAEL III 64
65.
POSTPARTUM CARE
RECOMMENDED
Routinely inspectthe birth
canal for lacerations
Inspect the placenta &
membranes for completeness
Early resumption of feeding
(<6 hours after delivery)
Massage the uterus –ensure
uterus is well contracted
Prophylactic antibiotics for
women with a 3rd or 4th
degree perineal tear
Early postpartum discharge
NOT RECOMMENDED
Manual exploration
of the uterus
Routine use of
icepacks over the
hypogastrium.
Routine oral
methylergometrine
BY: ROMMEL LUIS C. ISRAEL III 65
66.
Summary- Key
Points
Maternal andneonatal mortality
in the Philippines is still
unacceptably high
Prevention of postpartum
hemorrhage through interventions
like the use AMTSL will address
the #1 cause of maternal mortality
The evidence-based practices in
the EINC Protocol are lifesaving for
both mother and baby
BY: ROMMEL LUIS C. ISRAEL III 66
67.
Let us put
itinto
practice!
BY: ROMMEL LUIS C. ISRAEL III 67