Downloaded 30 times






















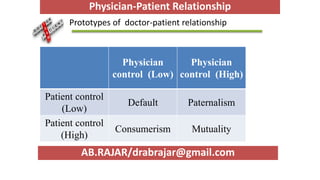















The document explores the physician-patient relationship, emphasizing its importance for excellent care and improved health outcomes. It discusses various relationship models, including paternalism, mutuality, and consumerism, as well as elements such as communication and decision-making that impact these relationships. The conclusion highlights the dynamic nature of these relationships and their direct correlation with health outcomes.























































































