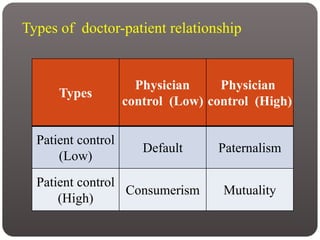
This document discusses the doctor-patient relationship and communication. It outlines Parsons' model of the sick role and doctor's role, and types of doctor-patient relationships including paternalism, mutuality, consumerism, and default. It covers influences on the relationship like time constraints, patient/doctor characteristics, and structural context. Effective communication skills, health literacy, consent, and partnerships in treatment decision making are also examined. The relationship has evolved from traditional paternalism to emphasize patient-centered care and shared decision making.