a physical examination is a crucial components of health assessments that involves a systematic and through examination of a patient's body to identify any abnormalities or signs of disease.
PHYSICAL EXAMINATION
INTRODUCTION-
Physical examinationis the process of collecting data or information to
detect clients health problems. It is the process of complete assessment of health status
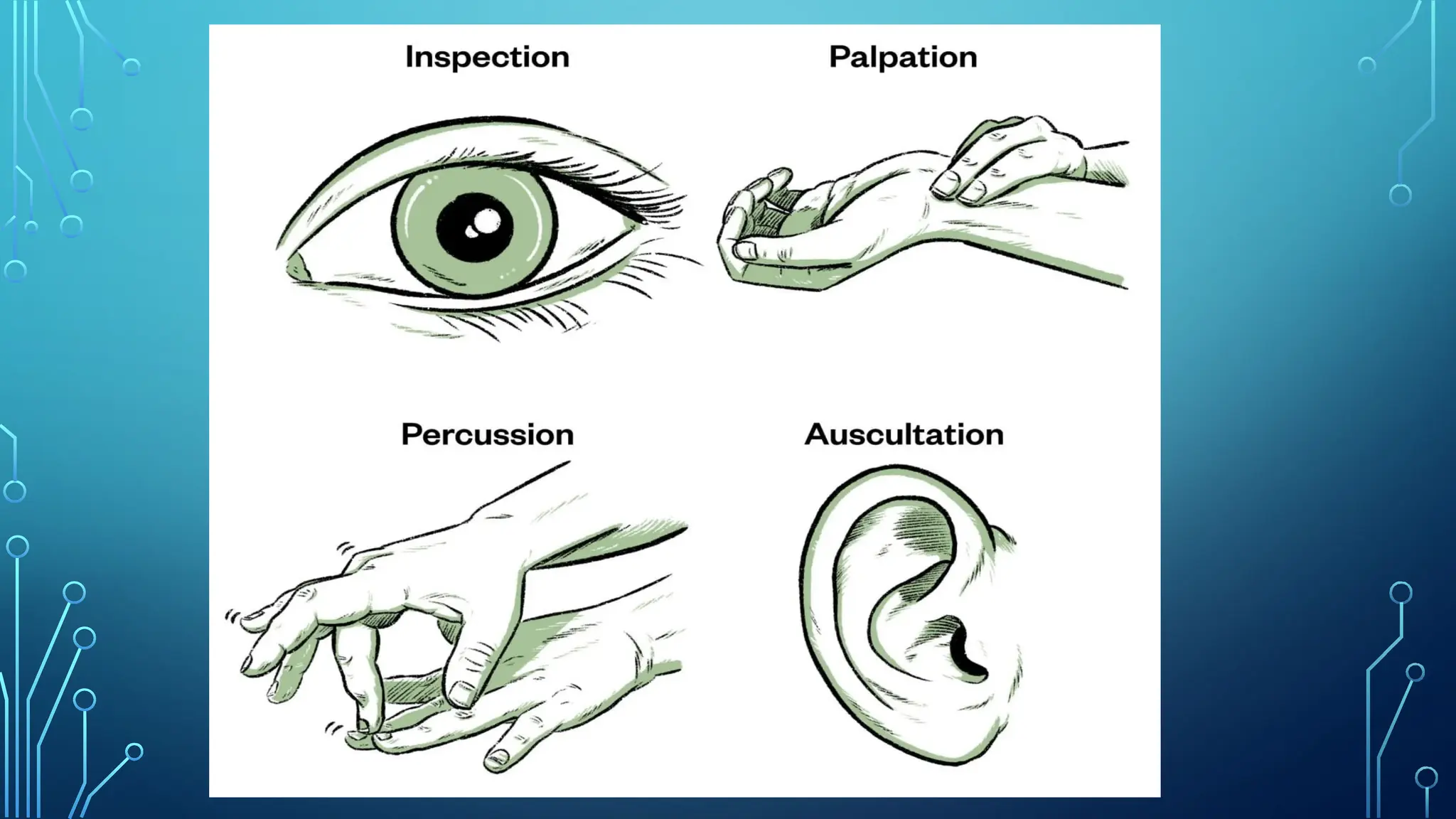
of a client through the use of various technique such as inspection ,palpation,
percussion and auscultation .
During the physical examination the nurse examines clients whole body to determine
any physical problems.
5.
DEFINITION
“Physical examination isdefined as a complete assessment
of a patient’s physical and mental status.’’
“Physical examination is defined as evaluation of the health
status of a patient through the use of inspection, palpation,
percussion and auscultation.”
6.
purpose
•To assess thephysical and mental purpose well being
of the clients.
•To determine the cause and extent of disease.
•To detect disease in it’s early stage.
•To contribute to the medical research.
•To determine the nature of the treatments.
7.
• To identifyhealth related needs and problems.
• To devise nursing care plan for the patient.
• To supplement and validate subjective data.
• To identify any changes in the condition of patients, any
improvement.
• To identify deviation in health patterns of the patient.
8.
PRINCIPLES
• During thephysical examination ,the nurse examines patient’s whole body or a
part of body as per need.
• Physical examination follows the history taking.
• Along with history taking and laboratory investigations, the physical examination
aids in identifying health problems and needs of the patients.
• The physical examination helps in making nursing diagnosis and nursing care
plan.
• During physical examination, objective data are collected to supplements and
validate the patient’s subjective data.
• Every person should have periodic physical examinations to identify any
deviation from normal health status.
INSPECTION
• It meanslooking at the body with naked eyes. Inspection
is the process of performing deliberate, purposeful
observations in a systematic manner.
• It involve observation of the colour of the skin, symmetry,
size, position and movements of body organs.
12.
A NURSE CANCOLLECT FOLLOWING INFORMATION BY PERFORMING
PHYSICAL EXAMINATION
GROOMING-
IT INVOLVES HYGIENE PRACTICES LIKE
SHOWERING, BRUSHING TEETH, AND HAIR
CARE, WHILE DRESSING INVOLVES
CHOOSING CLEAN, APPROPRIATE AND
WELL-FITTING CLOTHES FOR THE OCCASION.
• Body size,colour of skin and conjunctiva, symmetry of body organs,
movements.
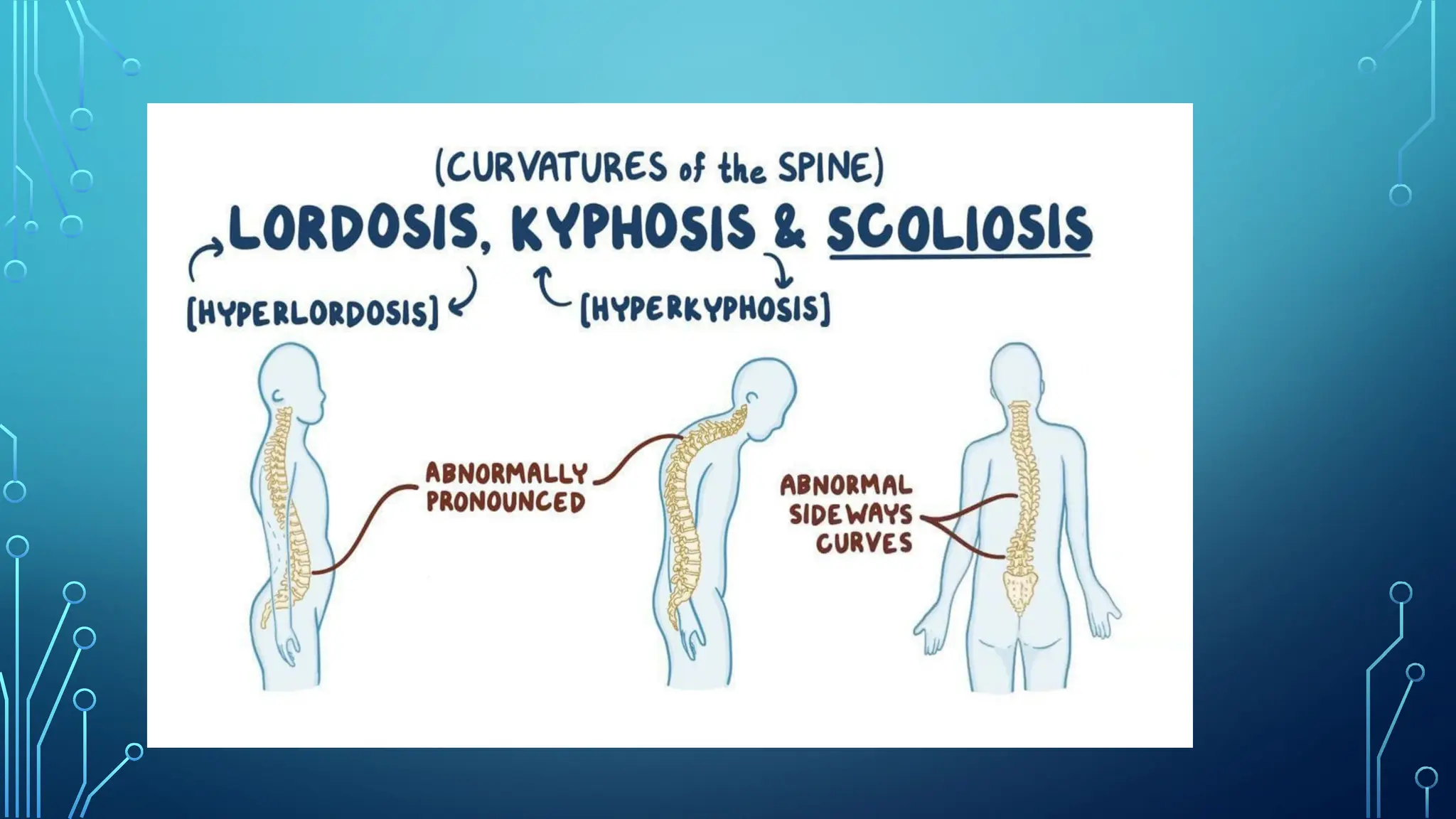
• Body posture: Any deviation from normal body posture like; kyphosis,
lordosis
• Any sign of presence of cyanosis, jaundice and anaemia.
• Presence of skin abrassions or skin rash.
19.
PRINCIPLES
• The followingprinciples should be kept in mind for making accurate
inspection-
• Make sure good lighting is available.
• Position and expose body part to view all surfaces.
• Provides privacy to the patients if require.
• Inspect each area for size, shape, colour, symmetry and proposition and find
out any deviations from normal.
• Use of direct lighting source to inspect body cavities.
• The environment should be comfortable and ventilated .
• Validate findings with the patients experience.
20.
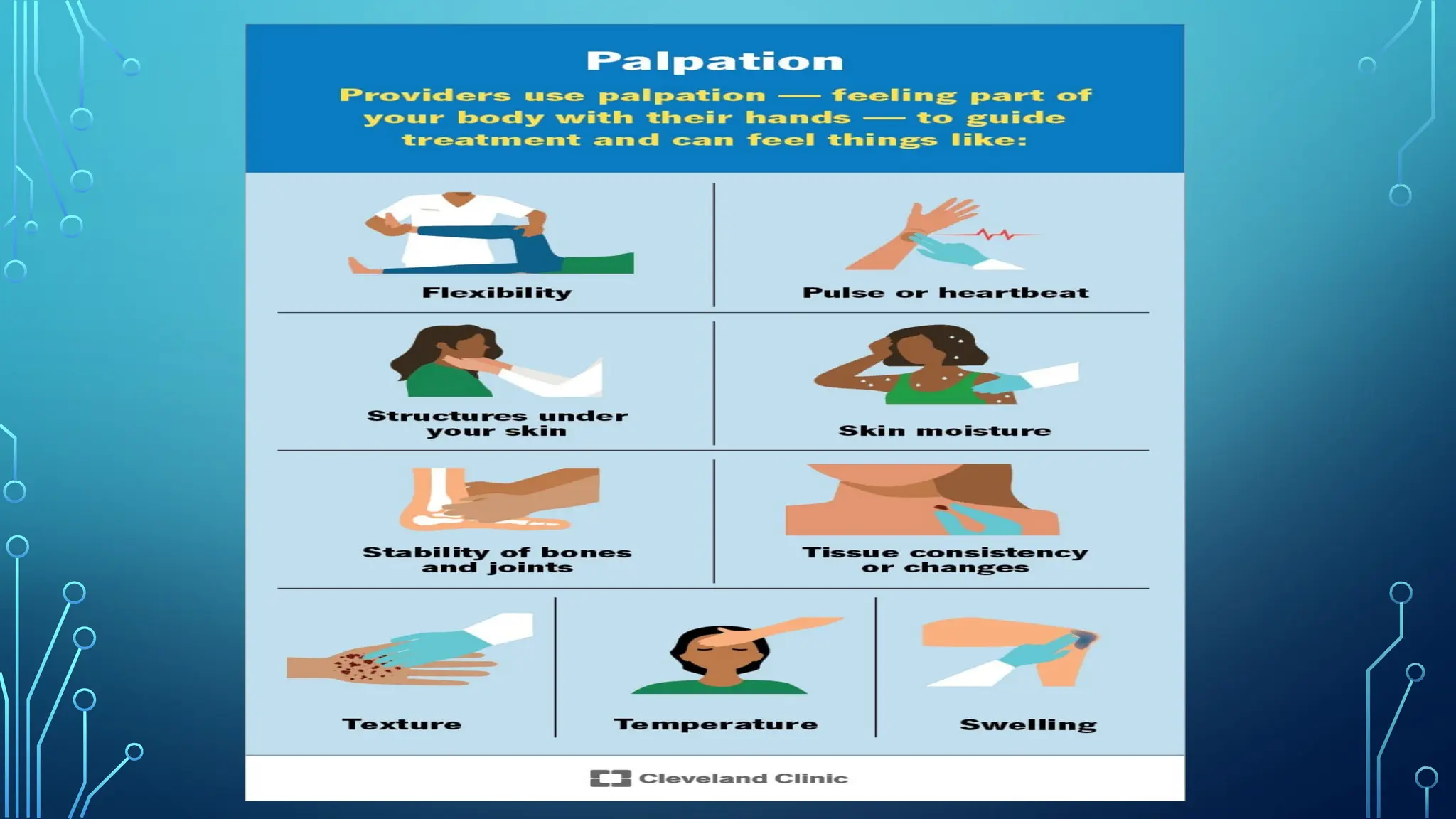
PALPATION
palpation uses thesense of touch. Palpation is an assessment
techniques in which the examiner feels with his/her fingers and
one or both hands. Through touch you make judgements about
expected and unexpected findings of the skins, tissue, muscle and
bones. The hands and fingers are sensitive parts and can assess
skin, temperature, texture(appearance), turgor(the skin’s
elasticity), moisture, swelling and tenderness.
22.
The following points
•The clients should be relaxed and comfortable.
• Palpation should be done with warm hands and short nails.
• Palpation should be proceed from light to deep.
• Palpation should be done slowly and gently.
• Fingertips should be used for palpation.
• For light palpation the hand is depressed about 1cm. And for deeper
palpation tissues are depressed about 4-5cm.
• Hand washing should be done before and after the procedure.
23.
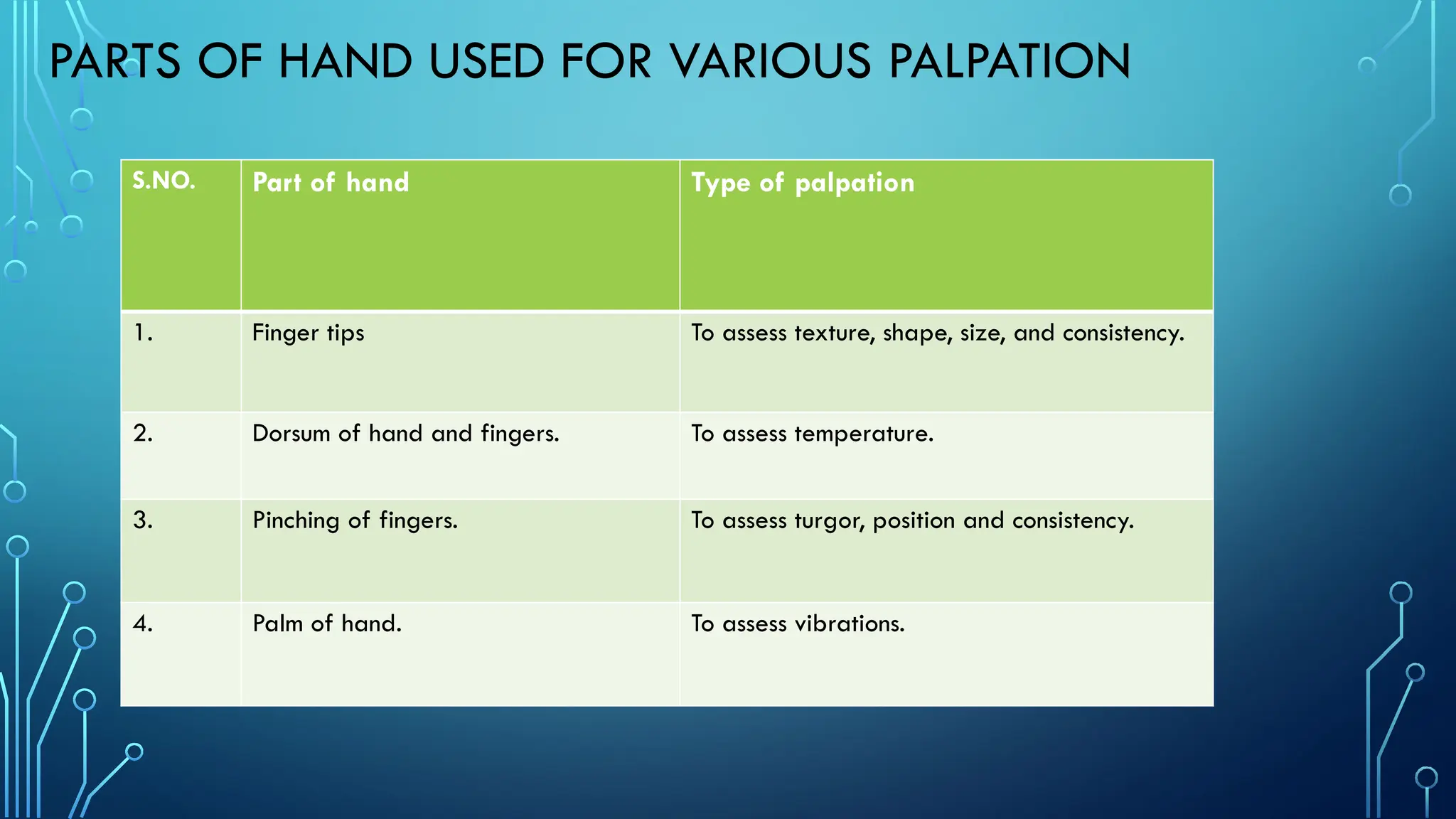
PARTS OF HANDUSED FOR VARIOUS PALPATION
S.NO. Part of hand Type of palpation
1. Finger tips To assess texture, shape, size, and consistency.
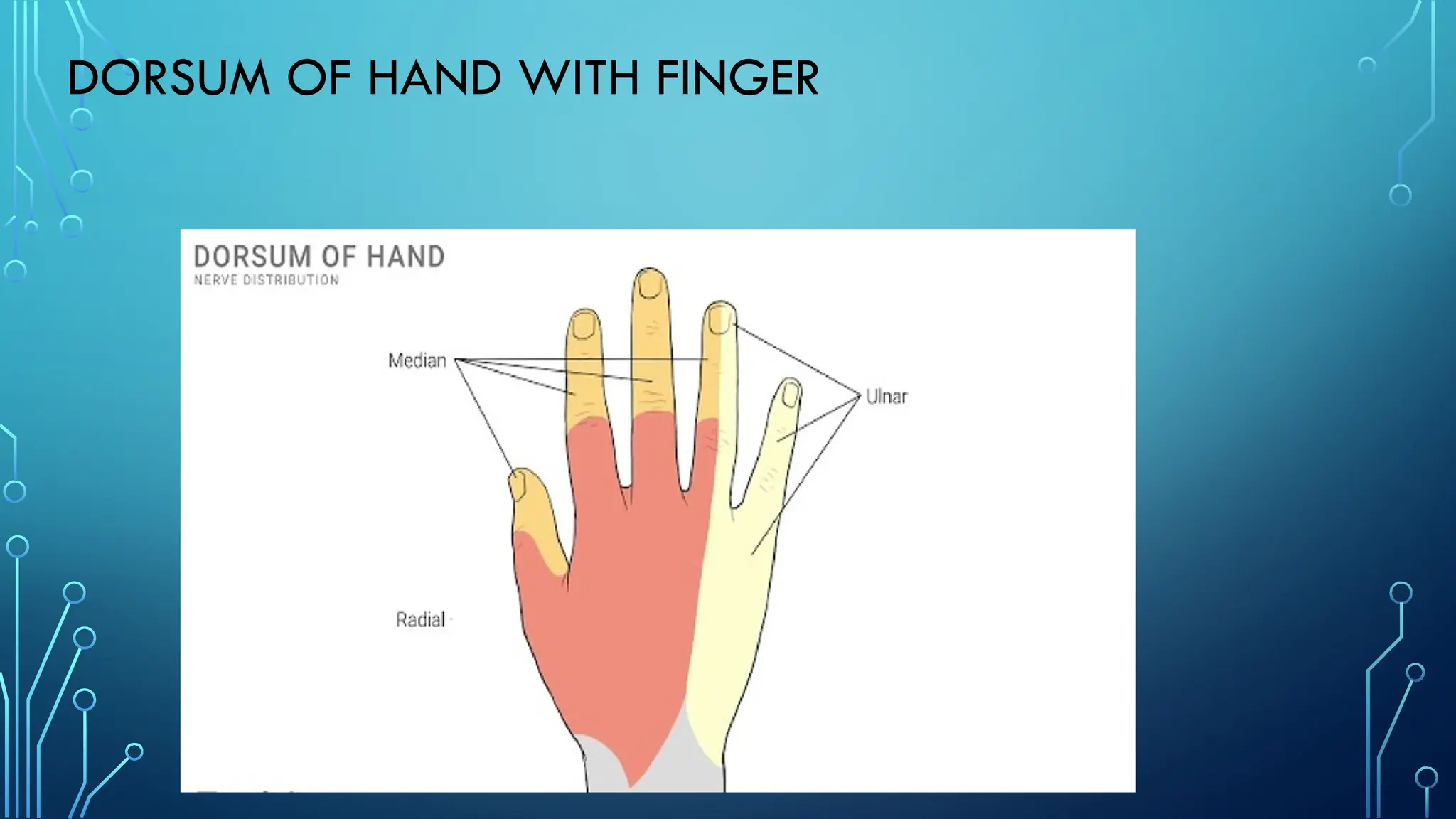
2. Dorsum of hand and fingers. To assess temperature.
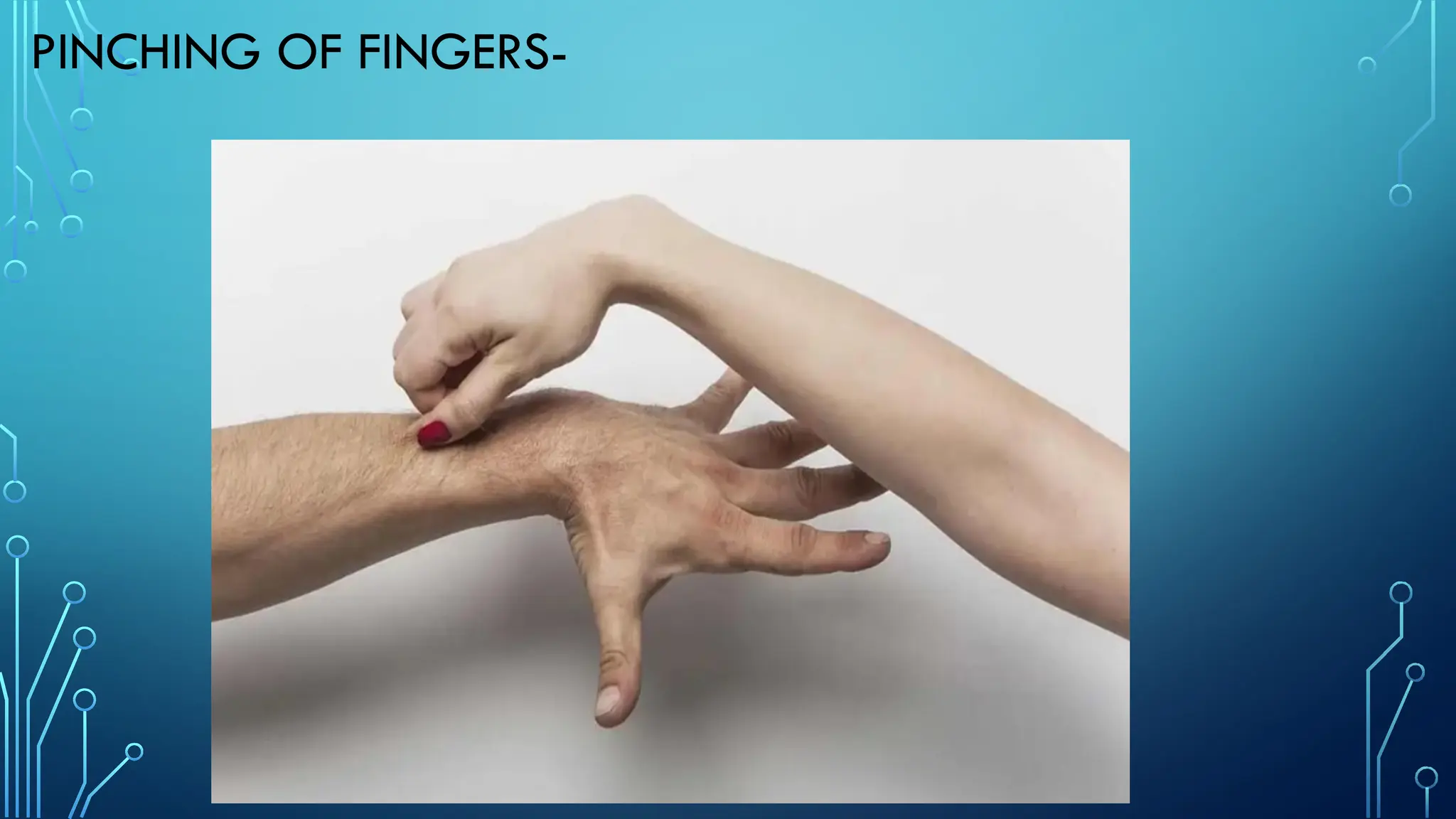
3. Pinching of fingers. To assess turgor, position and consistency.
4. Palm of hand. To assess vibrations.
TYPES OF PALPATION
Threetypes of palpation are-
•Light palpation
•Deep palpation
•Bimanual palpation
28.
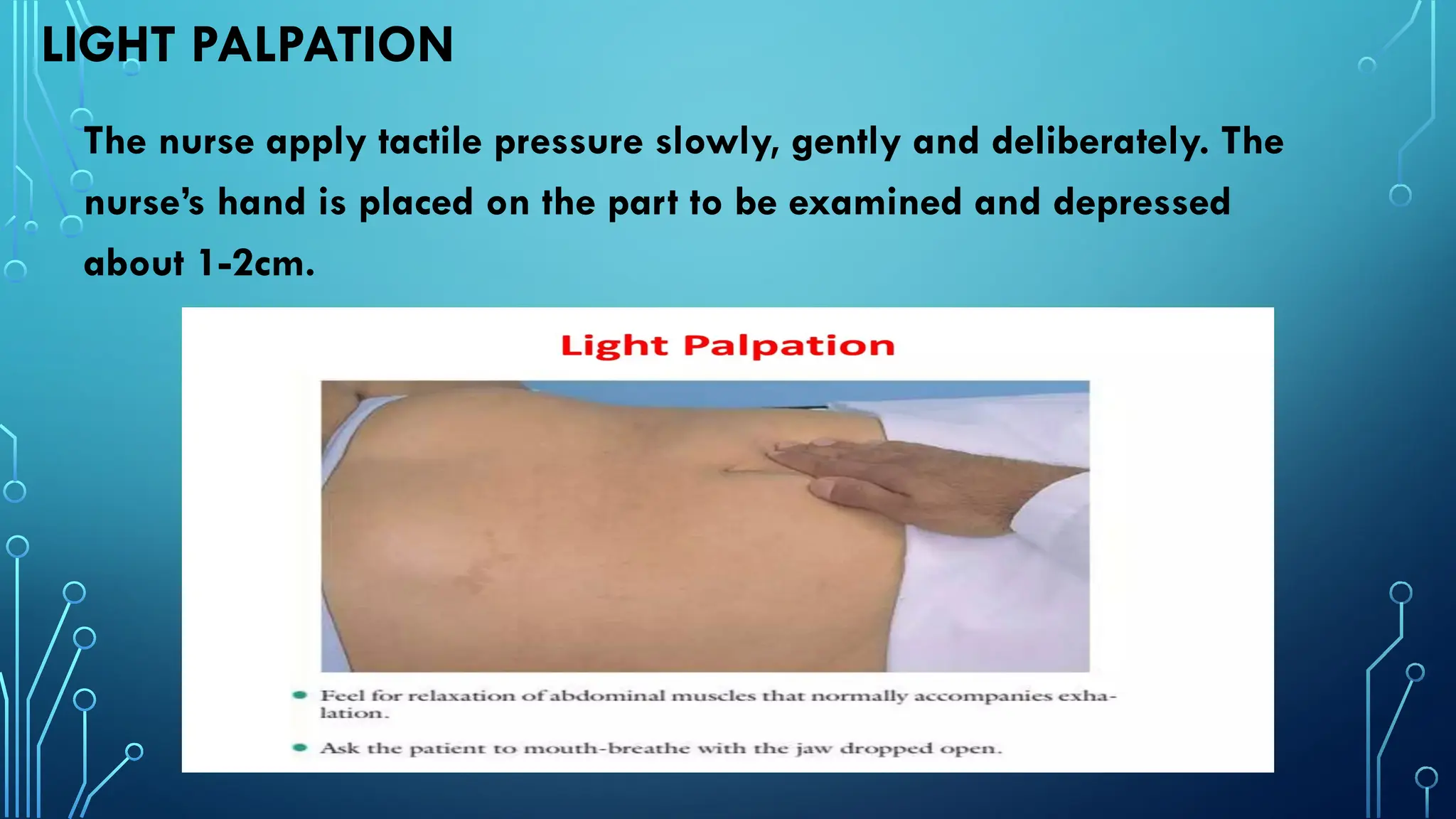
LIGHT PALPATION
The nurseapply tactile pressure slowly, gently and deliberately. The
nurse’s hand is placed on the part to be examined and depressed
about 1-2cm.
29.
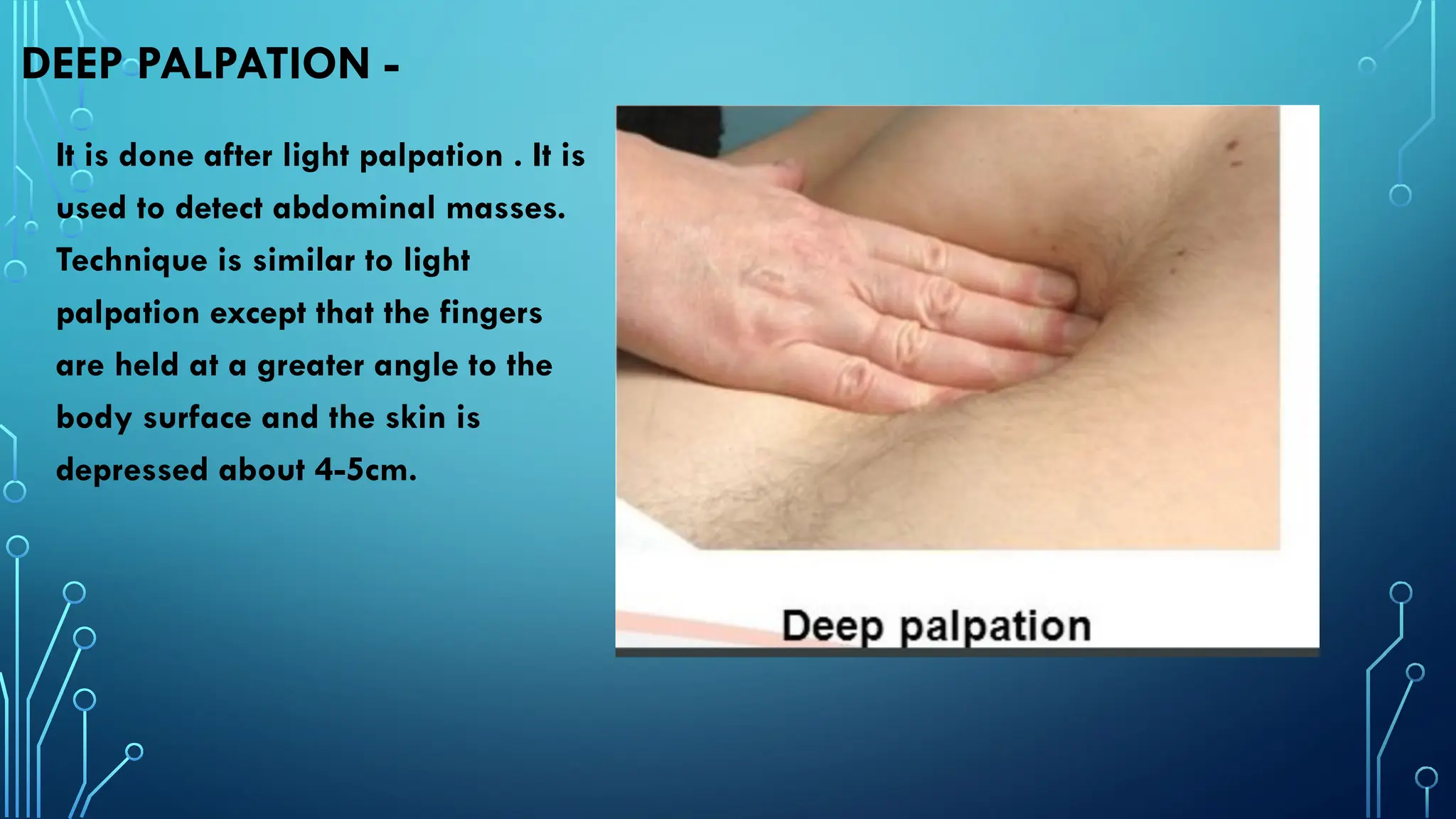
DEEP PALPATION -
Itis done after light palpation . It is
used to detect abdominal masses.
Technique is similar to light
palpation except that the fingers
are held at a greater angle to the
body surface and the skin is
depressed about 4-5cm.
30.
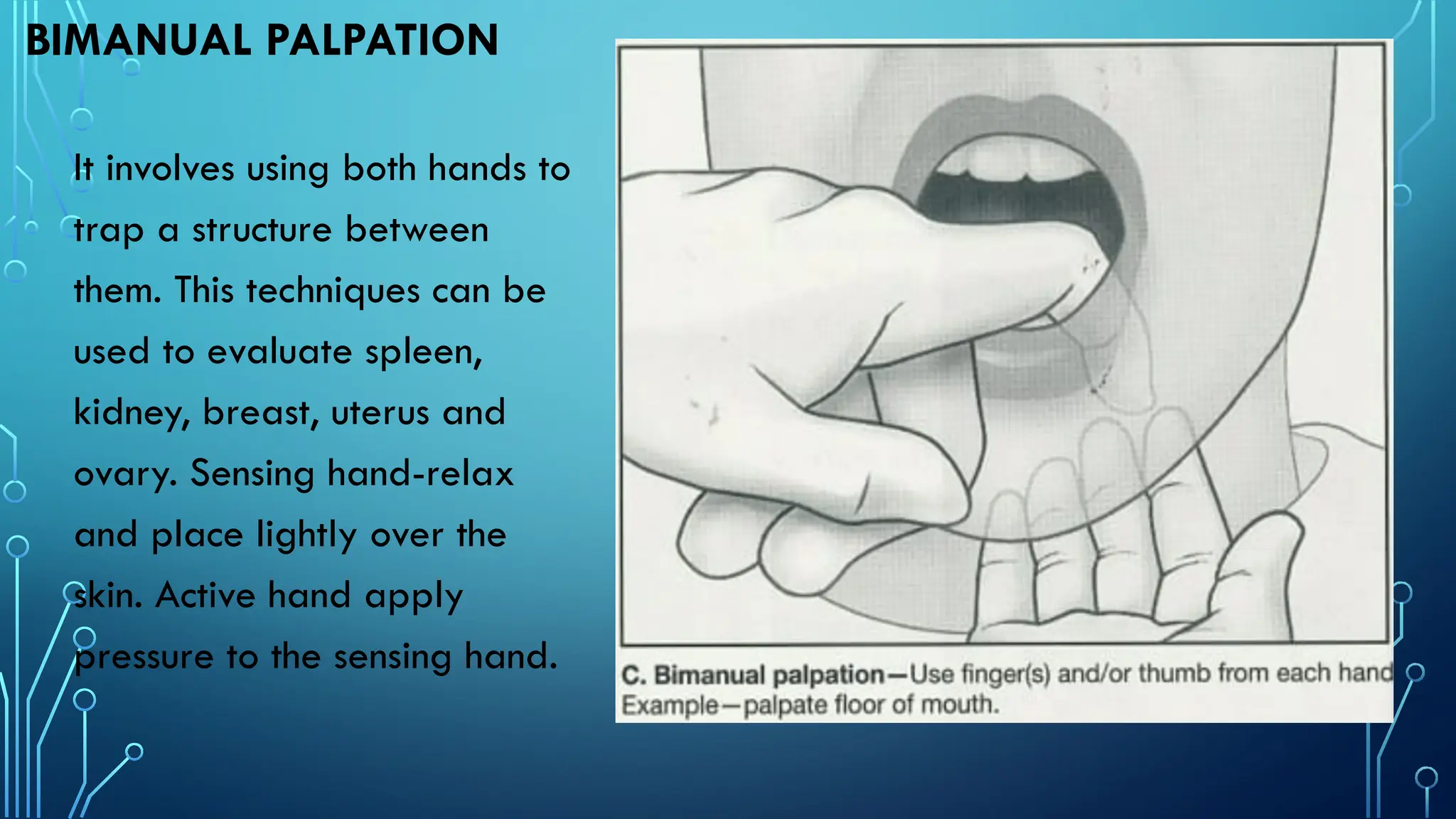
BIMANUAL PALPATION
It involvesusing both hands to
trap a structure between
them. This techniques can be
used to evaluate spleen,
kidney, breast, uterus and
ovary. Sensing hand-relax
and place lightly over the
skin. Active hand apply
pressure to the sensing hand.
31.
PERCUSSION
It means strikingtapping with fingers. Percussion
involve tapping with fingers. Percussion involve
tapping the skin with the fingertips to vibrate
underlaying tissues and organ. Percussion is the act of
striking one object against another to produce sound.
Percussion is used to assess the location, shape, size
and density of tissues.
32.
Body structure containingair, fluid and solid produces different sound
on percussion. A special instrument known as percussion hammer can
be used for this purpose.
Percussion on hand
33.
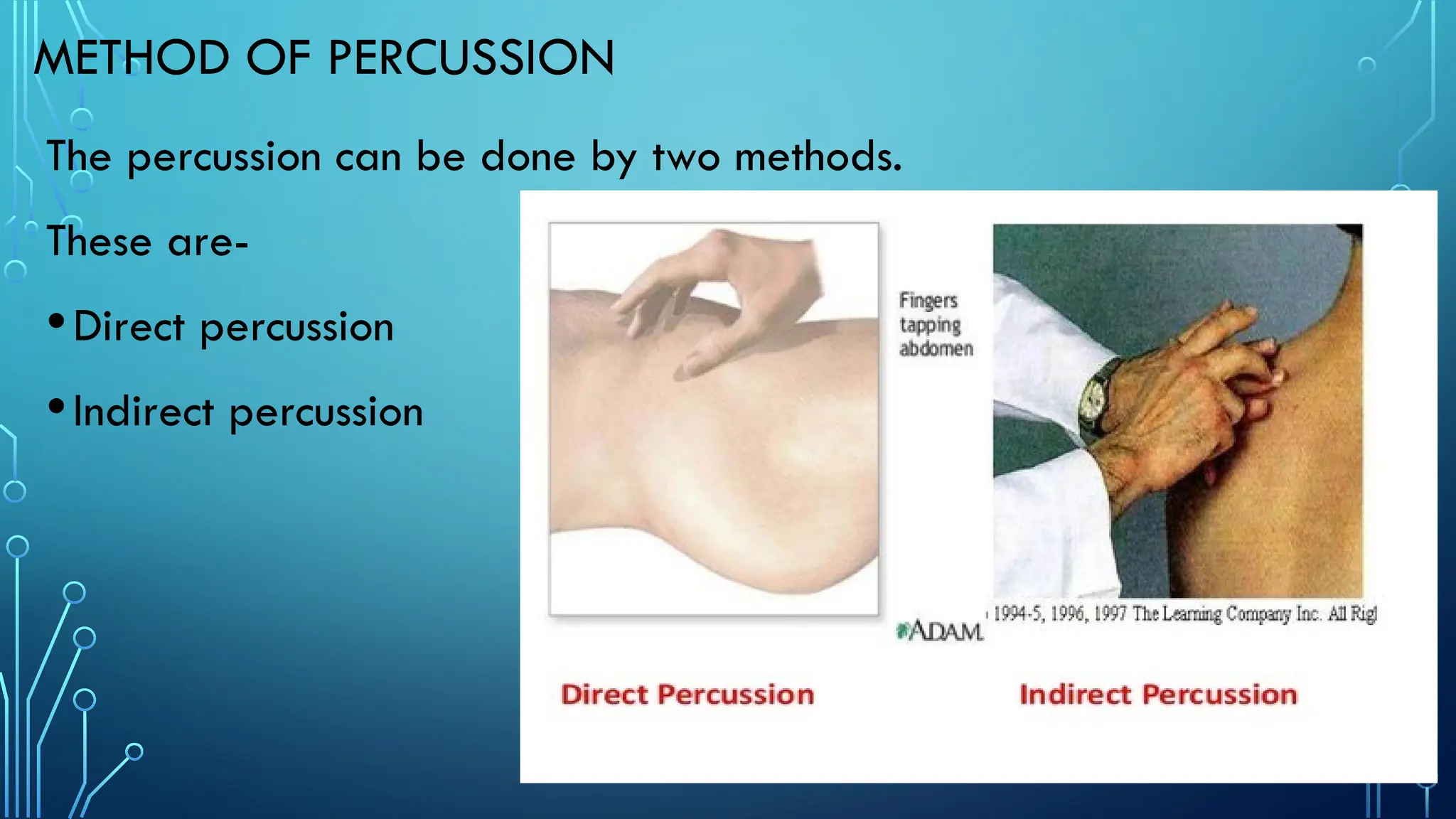
METHOD OF PERCUSSION
Thepercussion can be done by two methods.
These are-
•Direct percussion
•Indirect percussion
34.
DIRECT PERCUSSION-
Striking thebody surface directly with one or two fingers to
produce sound.
Indirect percussion-
Placing the middle finger of the non-dominant hand firmly
against the body surface and striking (tapping) the distal joint
of non-dominant finger with the middle finger of the dominant
hand.
35.
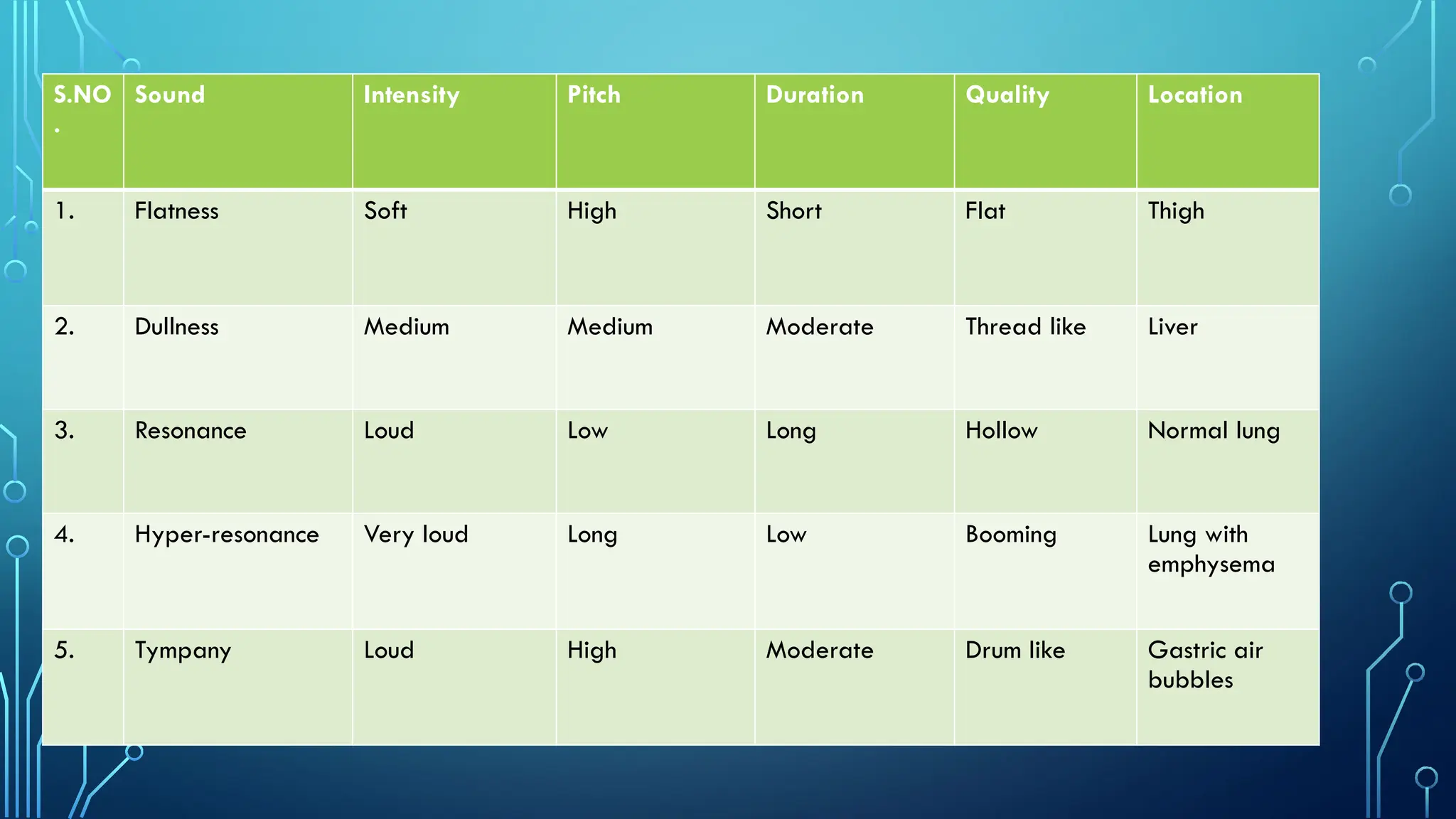
S.NO
.
Sound Intensity PitchDuration Quality Location
1. Flatness Soft High Short Flat Thigh
2. Dullness Medium Medium Moderate Thread like Liver
3. Resonance Loud Low Long Hollow Normal lung
4. Hyper-resonance Very loud Long Low Booming Lung with
emphysema
5. Tympany Loud High Moderate Drum like Gastric air
bubbles
36.
AUSCULTATION-
Auscultation is theact of listening the sound with a stethoscope
produced by the various body organs such as lungs, heart, GI
tract.
It reveals sound produced within the body and the blood vessels
such as heart beats, bowel sounds.
In auscultation sound can be listen directly by placing ear over
the area or with the help of stethoscope.
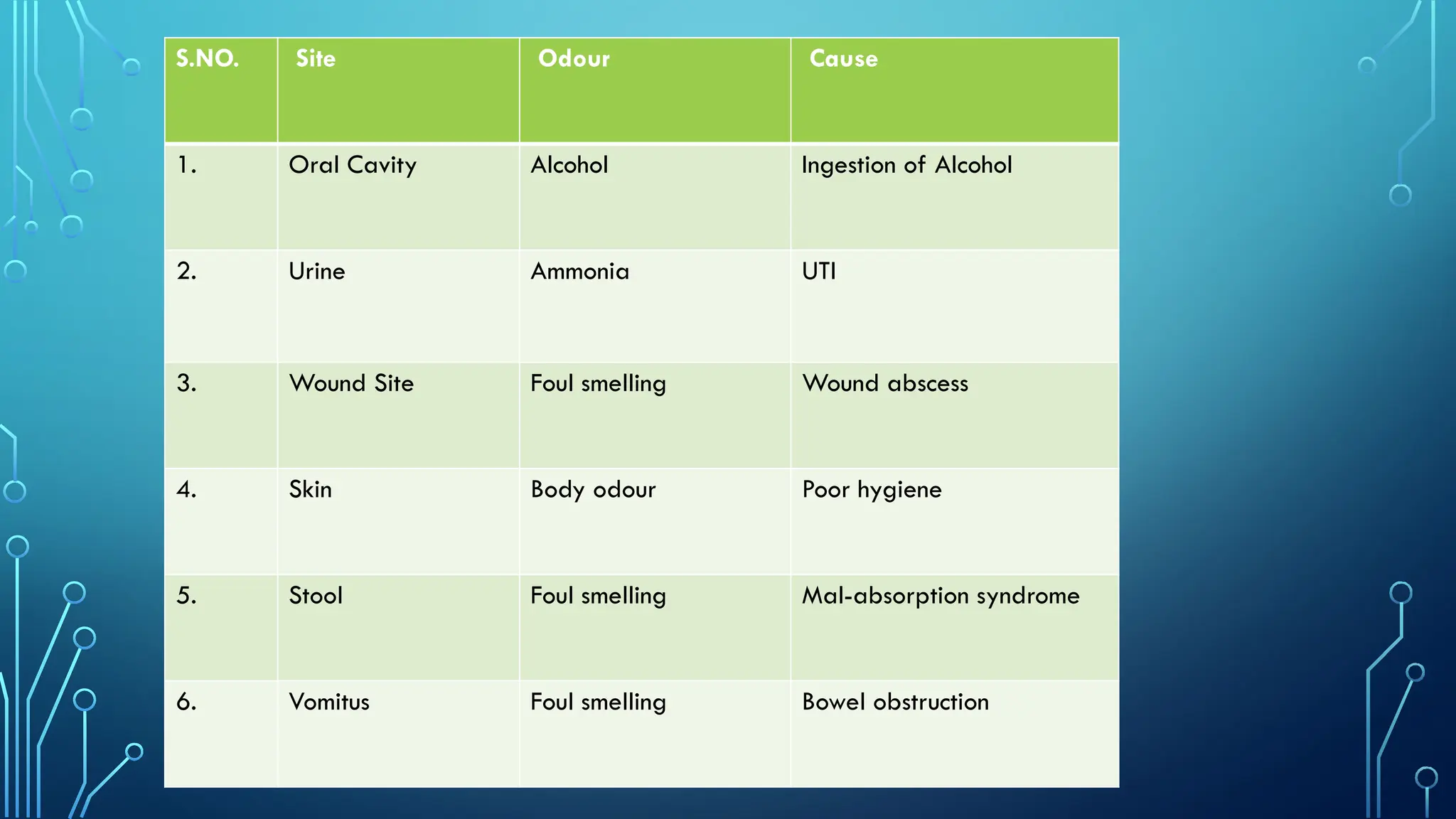
OLFACTION -
Olfaction isthe sense of smell. Olfaction helps to
detect abnormalities not recognized by other
means and this can help to detect serious
abnormalities.
39.
S.NO. Site OdourCause
1. Oral Cavity Alcohol Ingestion of Alcohol
2. Urine Ammonia UTI
3. Wound Site Foul smelling Wound abscess
4. Skin Body odour Poor hygiene
5. Stool Foul smelling Mal-absorption syndrome
6. Vomitus Foul smelling Bowel obstruction























![✅ CCleaner Pro Free Crack 6.34 + Activation Key [APRIL-2025]](https://cdn.slidesharecdn.com/ss_thumbnails/physicalexamination-250415070608-e7301bc1-250415080446-ea0ab5fb-thumbnail.jpg?width=640&height=640&fit=bounds)
![✅ Download CCleaner Pro Key 2025 with Crack [Latest]](https://cdn.slidesharecdn.com/ss_thumbnails/physicalexamination-250415070608-e7301bc1-250415082125-6d1be3de-thumbnail.jpg?width=640&height=640&fit=bounds)