Downloaded 160 times


![Study of [drug] over time
Visit us www.dentaltutor.in](https://image.slidesharecdn.com/pharmacokinetics-160610064959/85/Pharmacokinetics-6-320.jpg)
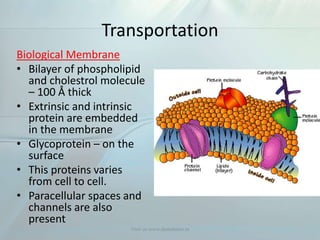
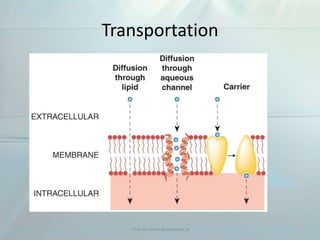


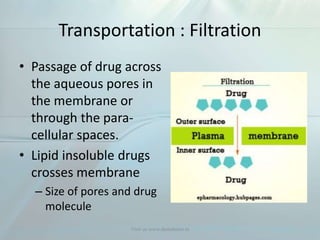


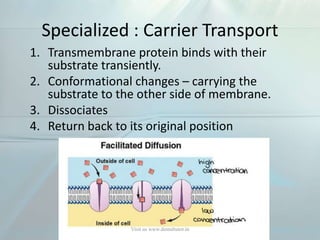

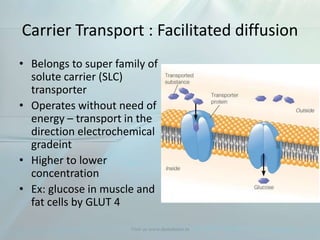
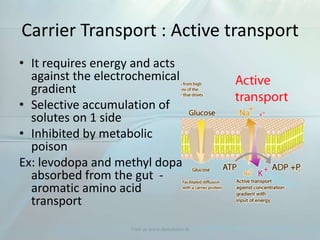











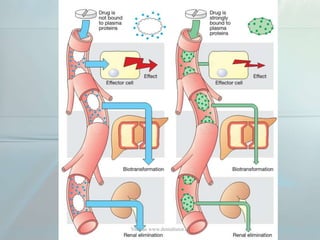




















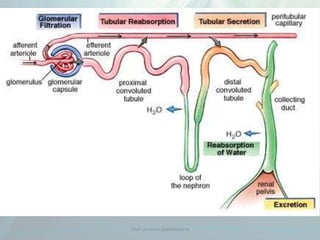









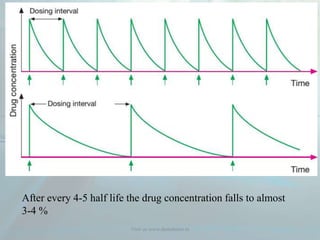
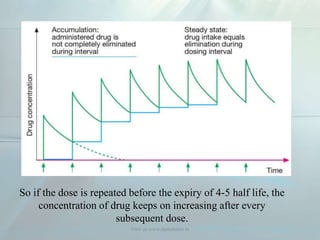









Clinical pharmacokinetics is the quantitative study of drug movement in, through, and out of the body. It involves the processes of absorption, distribution, metabolism, and excretion (ADME). Pharmacokinetics helps understand how the body affects a drug over time. Drugs are transported across biological membranes via passive diffusion, filtration, or specialized carrier transport systems. Once in circulation, drugs are distributed to tissues depending on factors like lipid solubility and plasma protein binding. The liver is the primary site of drug metabolism, which alters drugs through oxidation, reduction, hydrolysis, and conjugation to make them more polar and excretable. Understanding a drug's pharmacokinetics allows for individualization of drug therapy and














![Clinical Pharmacokinetics-I [half life, order of kinetics, steady state]](https://cdn.slidesharecdn.com/ss_thumbnails/clinicalpk-ihalflifeorderofkineticssteadystate-140217020044-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
















































































