This document discusses pharmacokinetics and membrane transport. It provides an overview of the following key points in 3 sentences:
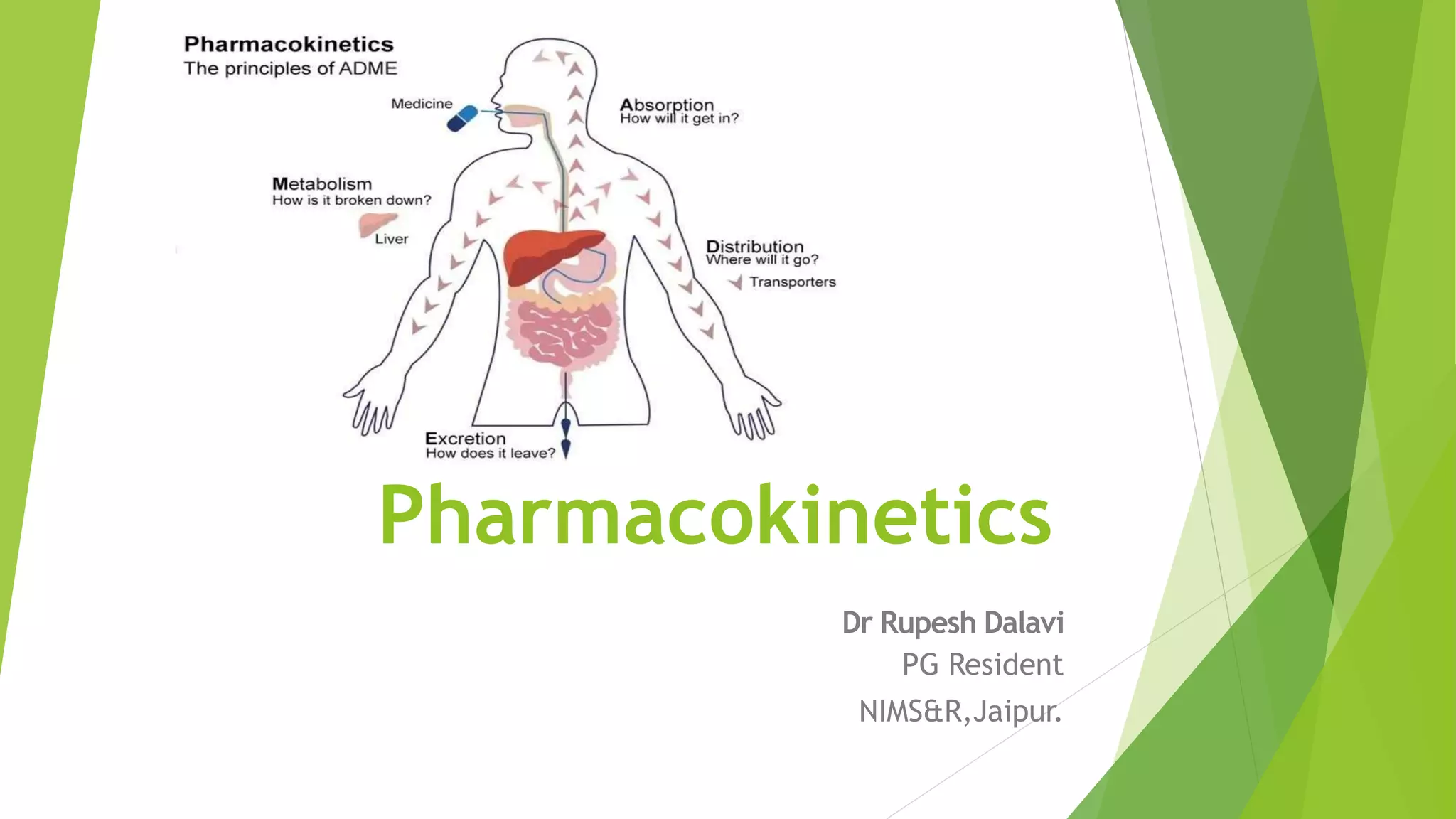
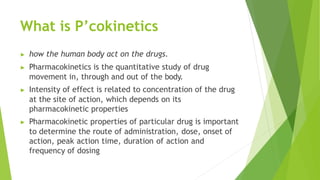
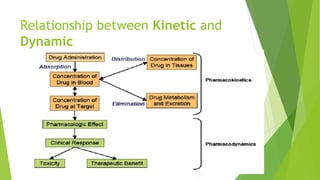
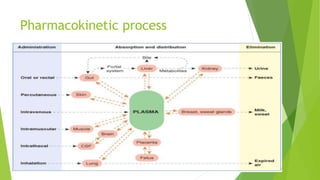
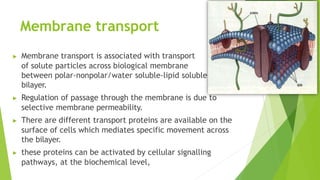
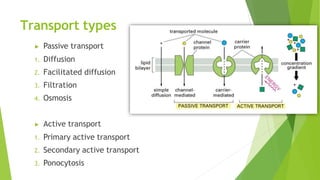
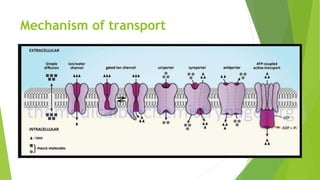
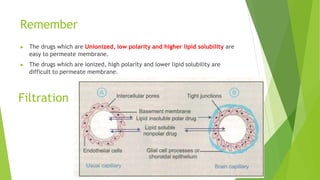
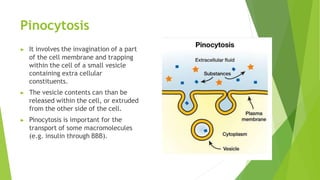
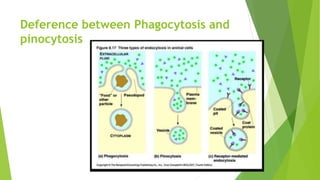
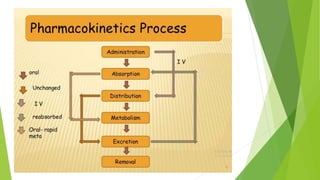
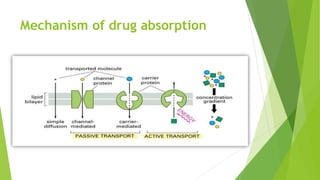
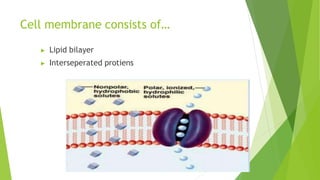
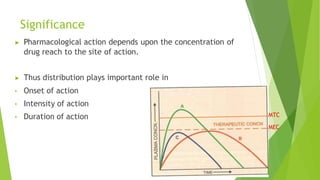
Pharmacokinetics studies how the body acts on drugs by quantifying drug movement in, through, and out of the body. The intensity of a drug's effect depends on its concentration at the site of action, which is determined by the drug's pharmacokinetic properties like absorption, distribution, metabolism and excretion. Membrane transport involves the passage of molecules like drugs across cell membranes, which can occur through passive diffusion or active transport utilizing transport proteins and cellular energy.






























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
