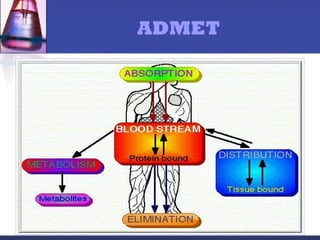
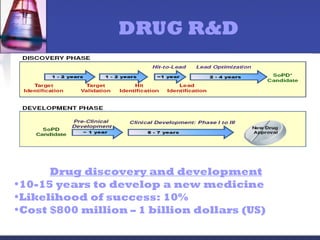
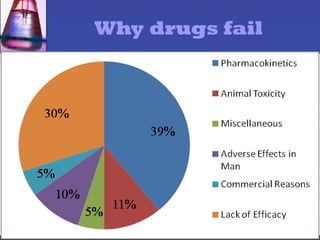
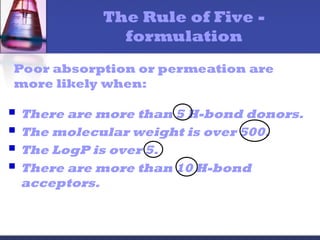
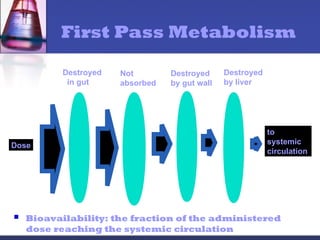
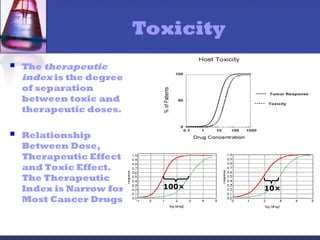
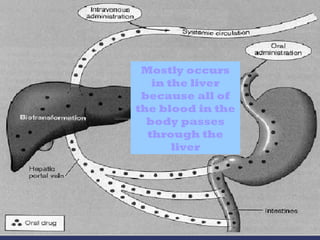
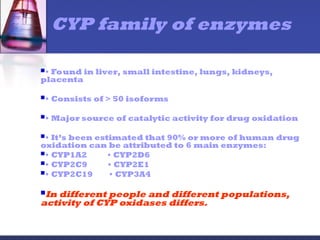
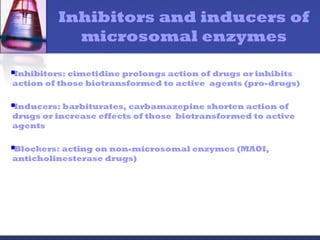
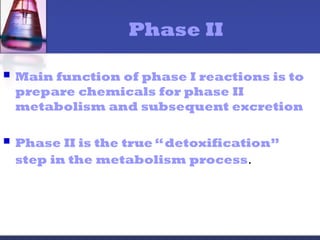
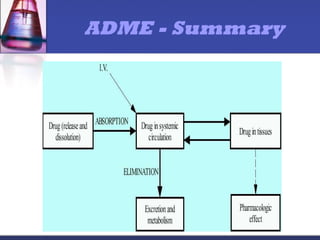
The document outlines the pharmacokinetics of drugs, detailing the processes of absorption, distribution, metabolism, and excretion (ADME). It emphasizes the significance of pharmacokinetics studies in drug development and the factors influencing drug efficacy and toxicity. Additionally, it discusses drug metabolism phases and the role of enzymes, particularly the cytochrome P450 family, in drug biotransformation.