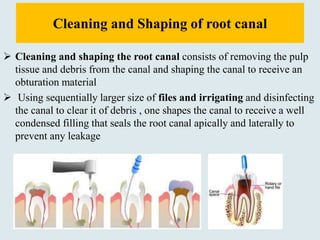
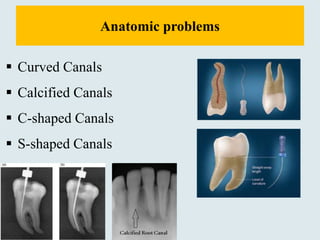
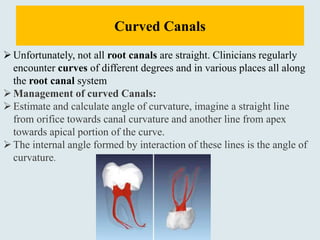
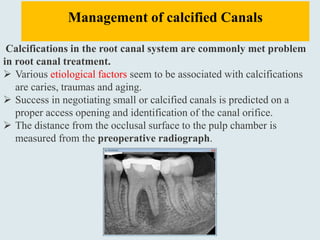
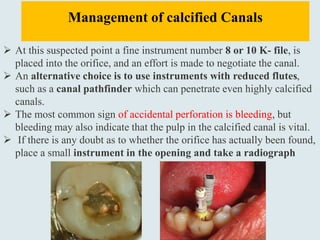
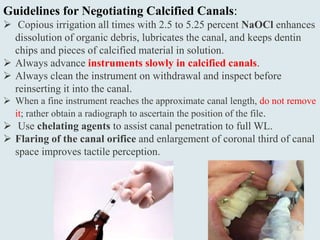
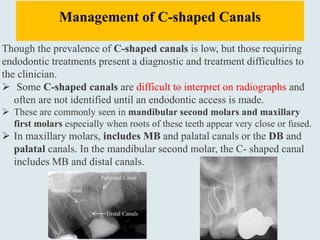
This document discusses special anatomic problems that can occur during canal cleaning and shaping, including curved canals, calcified canals, C-shaped canals, and S-shaped canals. It provides guidelines for managing each type of anatomic problem, such as using smaller files, pre-curving files, changing filing techniques, copious irrigation, and adjusting filing forces. Managing complex canal anatomies requires modified cleaning and shaping approaches to complete the endodontic procedure successfully.