PRINCIPLES OF CLEANINGAND
SHAPING
Mechanical Objectives:
• Aim to completely and centrally incorporate the original canal anatomy into the prepared shape.
• Goal: All canal surfaces should be mechanically prepared.
• Current techniques often fall short of this ideal.
• Important to preserve cervical and radicular dentin to maintain structural integrity.
• Minimizing dentin removal helps prevent root fractures.
Biologic Objective:
• Enlarged apical canals and finer irrigation needles allow deeper needle penetration.
• Deeper needle placement enhances debridement and disinfection of the root canal system.
3.
ENDODONTIC INSTRUMENTS
1. K-TypeInstruments
• Include K-files and K-reamers.
• Made by twisting square or triangular blanks.
• K-files: More flutes per mm, suited for filing motion.
• Reamers: Fewer flutes, more suited for twisting motion.
• Triangular cross-sections are more flexible than square ones.
• Reamers are less commonly used today.
4.
ENDODONTIC INSTRUMENTS
2. H-TypeInstruments (Hedström Files)
• Made by milling round stainless-steel blanks.
• Very efficient in translational (filing) motion.
• Features:
• Positive rake angle
• Sharp, aggressive cutting edges
• Can thread into canal during rotation (caution).
• Higher stress concentration when bent → risk of fracture.
5.
ENDODONTIC INSTRUMENTS
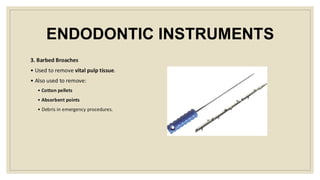
3. BarbedBroaches
• Used to remove vital pulp tissue.
• Also used to remove:
• Cotton pellets
• Absorbent points
• Debris in emergency procedures.
6.
LOW-SPEED ENGINE-DRIVEN INSTRUMENTS
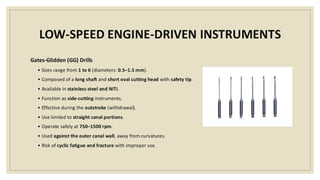
Gates-Glidden(GG) Drills
• Sizes range from 1 to 6 (diameters: 0.5–1.5 mm).
• Composed of a long shaft and short oval cutting head with safety tip.
• Available in stainless steel and NiTi.
• Function as side-cutting instruments.
• Effective during the outstroke (withdrawal).
• Use limited to straight canal portions.
• Operate safely at 750–1500 rpm.
• Used against the outer canal wall, away from curvatures.
• Risk of cyclic fatigue and fracture with improper use.
7.
LOW-SPEED ENGINE-DRIVEN INSTRUMENTS
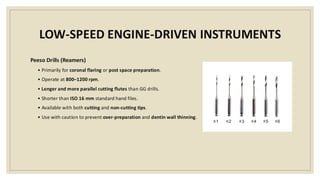
PeesoDrills (Reamers)
• Primarily for coronal flaring or post space preparation.
• Operate at 800–1200 rpm.
• Longer and more parallel cutting flutes than GG drills.
• Shorter than ISO 16 mm standard hand files.
• Available with both cutting and non-cutting tips.
• Use with caution to prevent over-preparation and dentin wall thinning.
8.
STEPS OF CLEANINGAND SHAPING
1. Coronal Preflaring
• Extension of access cavity into coronal part of the root canal.
• Tools:
• Gates Glidden drills
• NiTi instruments
• Orifice shaping rotaries (single-instrument systems).
• Benefits:
• Reduces risk of working length changes.
• Facilitates straighter access for instruments.
• Improves irrigation effectiveness.
9.
STEPS OF CLEANINGAND SHAPING
2. Patency File
• Use of a small K-file (#10 or #15) extended slightly beyond the apical foramen.
• Recommended for most rotary instrumentation techniques.
• Functions:
• Clears apical debris.
• Maintains accurate working length.
• Improves overall canal cleanliness.
• Note: Does not increase post-op symptoms when used correctly.
10.
WORKING LENGTH DETERMINATION
Devices
•Traditional methods:
• Radiographs, tactile sensation, moisture on paper points, root morphology.
• Electronic Apex Locator (EAL):
• Highly accurate for determining working length.
• Apical resorption does not affect accuracy.
• Early generations were affected by canal contents and irrigants.
• Caution: Avoid use in pacemaker patients unless cleared by cardiologist.
11.
CLEANING AND SHAPINGTECHNIQUES
1. Standardized Technique
• All instruments used to same working length.
• Canal shape dictated by instrument shape.
• Limited by instrument standardization.
2. Step-Back Technique
• Larger files used in steps 0.5–1 mm shorter than previous.
• Creates flared canal with 0.05–0.10 taper.
• Reduces preparation errors, especially in curved canals.
12.
CLEANING AND SHAPINGTECHNIQUES
3. Step-Down Technique
• Shape coronal portion first, then apical instrumentation.
• Minimizes extrusion of necrotic debris.
4. Crown-Down Technique
• Emphasizes coronal flaring first, then apical shaping.
• Working length determined after coronal flaring.
• Use of stainless-steel K-file to explore apical area.
• Avoid excessive wall contact to prevent blockage.
13.
CLEANING AND SHAPINGTECHNIQUES
5. Balanced Forces Technique
• Minimizes canal aberrations.
• Best canal-centering hand technique.
• Involves 3 steps:
o 90° clockwise to engage dentin
o 180–270° counterclockwise to cut
o 360–720° clockwise to remove file
6. Rotary Instrumentation
• Requires glide path of size #15–20 K-file.
• Needs copious irrigation and frequent recapitulation.
14.
NiTi ROTARY TECHNIQUES
◦Crown-Down
• WL determined after pre-enlargement.
• Glide path secured first with K-files.
◦ Single Length (e.g., ProTaper)
• No crown-down step.
• Follows specific file sequence:
S1/S2 → re-irrigation → WL confirmation → Finishing files.
15.
DISINFECTION OF THEROOT CANAL
SYSTEM
Objectives of Irrigation:
• Mechanical:
1. Flush out debris
2. Lubricate canal
3. Prevent or remove smear layer
• Chemical:
1. Dissolve organic/inorganic tissue
2. Kill microorganisms
• Biologic: Overall canal disinfection
16.
DISINFECTION OF THEROOT CANAL
SYSTEM
Effectiveness Depends On:
• Mechanical: Streaming forces throughout the canal
• Chemical: Concentration, contact area, and duration
Ideal Properties of Irrigants
• Kill bacteria in planktonic and biofilm states
• Inactivate endotoxins
• Be non-toxic to vital tissues
• Avoid anaphylactic reactions
17.
DISINFECTION OF THEROOT CANAL
SYSTEM
Factors affecting irrigation efficiency:
1. Needle penetration depth
2. Canal diameter
3. Needle size and design (e.g., 30-gauge NiTi needle for curved canals)
4. Irrigation pressure (narrow needles = higher pressure/velocity)
5. Viscosity of the irrigant
6. Velocity at the needle tip
7. Needle tip type and orientation
• Side-vented or double side-vented → safer & better cleaning
• Closed-end tips → prevent apical extrusion
18.
Sodium Hypochlorite (NaOCl)
•Most commonly used endodontic irrigant
• Strong antibacterial agent
• Dissolves necrotic/vital pulp tissue, organic dentin & biofilms
• Used in 0.5%–6% concentrations
• Higher concentrations:
• Better at tissue dissolution
• More effective against E. faecalis & C. albicans
• More toxic
• Lower concentrations in higher volumes can be equally effective
19.
Sodium Hypochlorite (NaOCl)
Toxicityand Accidents
• Extrusion beyond apex can cause:
• Severe pain, edema, bleeding, ecchymosis
• Possible paresthesia, infection, or sinus irritation
• Management:
• Inform patient
• Pain control: local anesthesia, analgesics
• Cold compress (first day), then warm compresses & rinses
• Daily follow-up
• ABs & antihistamines not obligatory
• Corticosteroid use is controversial
20.
Chlorhexidine (CHX)
• Lesseffective than NaOCl for tissue dissolution
• More effective than saline as final rinse
As Intracanal Medicament
• Comparable/better than Ca(OH)₂ against E. faecalis
• Helps prevent root resorption and bacterial regrowth
• Works as gel or liquid
Other Uses
• Helps prevent bacterial coronal penetration
• Inhibits MMPs → improves dentin bond stability
21.
Ethylenediamine Tetraacetic Acid(EDTA)
• Removes inorganic part of smear layer
• Must be combined with NaOCl to eliminate organic components
• Effective in <1 min contact time
• Overuse or sequential NaOCl use can cause dentin erosion
EDTA Use Protocol
• Used after cleaning/shaping, for ~1 minute
• Can be ultrasonically activated for deeper penetration
• Should not be heated — heat reduces calcium-binding ability
Interaction with NaOCl
• Should be used separately
• Alternate regimen with copious NaOCl rinse after EDTA
• Avoid prolonged or combined exposure to prevent erosion
22.
INTRACANAL MEDICATIONS
Purpose ofIntracanal Medications
• Prevent bacterial regrowth between appointments.
• Provide continued disinfection.
• Act as a physical barrier inside the root canal system.
Calcium Hydroxide (Ca(OH)₂)
◦The most commonly used.
◦ 24-hour contact needed for complete elimination of E. faecalis.
• Application:
• Mixed with sterile water or saline.
• Placed using Lentulo spiral.
• Mixture must be moist but not overly dry.
• Used for:
• Apexification in immature necrotic teeth.
• Revascularization as an alternative to antibiotic pastes.
• Limitations:
• Incomplete removal (residues remain).
• Interferes with root canal sealers.
• Not fully effective against E. faecalis and Candida albicans.
25.
CRITERIA TO EVALUATECLEANING
AND SHAPING
What is a Well-Shaped Canal?
◦ Free of procedural errors.
◦ Achieves effective disinfection.
◦ Preserves as much natural tooth structure as possible.
26.
SIGNS OF PROCEDURALMISHAPS
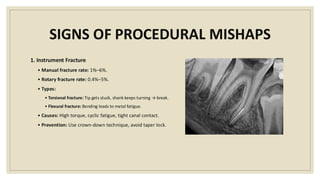
1. Instrument Fracture
• Manual fracture rate: 1%–6%.
• Rotary fracture rate: 0.4%–5%.
• Types:
• Torsional fracture: Tip gets stuck, shank keeps turning → break.
• Flexural fracture: Bending leads to metal fatigue.
• Causes: High torque, cyclic fatigue, tight canal contact.
• Prevention: Use crown-down technique, avoid taper lock.
27.
SIGNS OF PROCEDURALMISHAPS
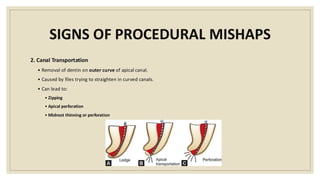
2. Canal Transportation
• Removal of dentin on outer curve of apical canal.
• Caused by files trying to straighten in curved canals.
• Can lead to:
• Zipping
• Apical perforation
• Midroot thinning or perforation
28.
SIGNS OF PROCEDURALMISHAPS
3. Perforation Types
• Strip perforation: Furcation area in multirooted teeth (“danger zone”).
• Curvature-related perforation: At curved canals.
• Apical perforation: Through the apex.
4. Blockage
• Canal becomes blocked by:
• Compacted debris.
• Pulp remnants.
• Broken file or filling materials.
29.
SIGNS OF PROCEDURALMISHAPS
5. Instrumentation Errors
• Ledge formation: Artificial step or shelf in canal wall.
• Transportation: Shifting canal end to a wrong location.
• Minor, Moderate, or Severe
• Zipping: Apical shape changed from round to teardrop/hourglass.
• Perforation: Unintended opening into periodontal ligament (PDL).