1) Determining if a clinically unstable infant truly has an infection remains challenging in neonatal sepsis evaluation and management.
2) Advances like heart rate characteristics monitoring and new sepsis biomarkers show promise for earlier infection detection, while molecular techniques may reduce pathogen identification time.
3) Antibiotic-resistant infections require less common drugs like linezolid, daptomycin, ciprofloxacin, and colistin, though safety data in neonates is limited; prevention focuses on hand hygiene and early catheter removal.

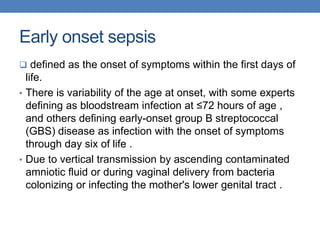
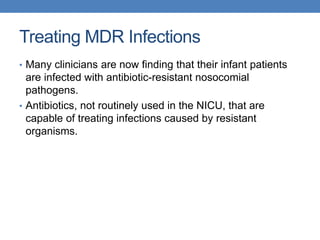
![probiotic
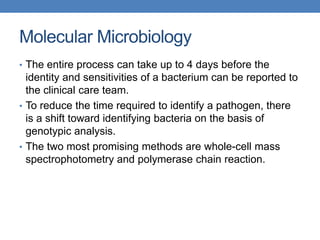
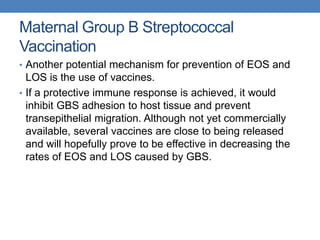
• in a 2014 systematic review of trials in preterm infants <37
weeks gestation or birth weight <2500 g using
preparations that contained bacterial strains
of Lactobacillus alone or in combination
with Bifidobacterium :
• Infants who received probiotics versus controls were less
likely to develop severe NEC (stage II or higher) (relative
risk [RR] 0.43, 95% CI 0.33-0.56) 20 studies.
• Infants who received probiotics had a lower mortality rate
(RR 0.65, 95% CI 0.52-0.81)17 studies.
• There was no difference in the rate of nosocomial sepsis
between infants who received probiotics and controls (RR
0.91, 95% CI 0.80-1.03). 19 studies.](https://image.slidesharecdn.com/futuredirectionsinneonatalsepsis-181106125639/85/Future-directions-in-neonatal-sepsis-29-320.jpg)





































![Sepsis neonatal [autoguardado]](https://cdn.slidesharecdn.com/ss_thumbnails/sepsisneonatalautoguardado-170318103240-thumbnail.jpg?width=640&height=640&fit=bounds)



































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













