• Disease spreadin the abdomenand pelvis generally occurs in
predictable pattern in relation to anatomic landmarks and fascial
planes
• The abdominal cavity traditionally devided into
peritoneal,retroperitoneal,and pelvic extraperitoneal spaces
• Pathalogic conditions differ in terms of pathways of disease spread
simple fluid –tracks along fascial planes, respect anatomical boundaries.
Fluid from ANP – destroy fascial planes, resulting in transfascial spread ,did not
respect anatomical boundaries
Neoplastic –multiple pathways with propensity for spread to noncontiguous sites.
4.
MODELS
1)TRADITIONAL /PERITONEAL BASEDMODEL :intraperitoneal & extraperitoneal
• localize disease processes and D/D
2)HOLISTIC MODEL /SUBPERITONEAL APPROACH :
Peritoneal cavity (no organs ),subperitoneal spaces
(abdominopelvic viscera & mesteric derivatives) & extraperitoneal spaces
• illustrates disease spread
3)MESENTERIC AND NON MESENTERIC DOMAINS MODEL:
Mesenteric domain- Mesentry and all digestive organs from GE junction to level of Mesorectum
Non mesenteric domain –GU organs ,great vessels ,MSK frame
• newer concept for surgical planning
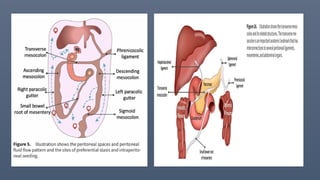
ANATOMY
• PERITONEAL LIGAMENTS
•two layers of visceral peritoneum doubled back on themselves.
• Organs and the other structures in peritoneal cavity to abdominal wall
• Conduit for BVs,Nerves,lymphatic vessels to enter and exit the organs
• Conduit and barrier for disease spread
• Mesentery –bowel
• Omentum –stomach
13.
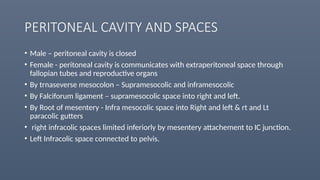
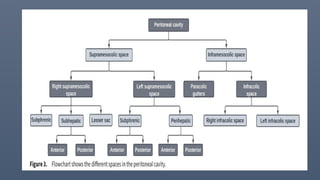
PERITONEAL CAVITY ANDSPACES
• Male – peritoneal cavity is closed
• Female - peritoneal cavity is communicates with extraperitoneal space through
fallopian tubes and reproductive organs
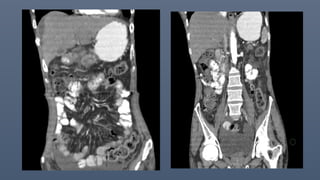
• By trnaseverse mesocolon – Supramesocolic and inframesocolic
• By Falciforum ligament – supramesocolic space into right and left.
• By Root of mesentery - Infra mesocolic space into Right and left & rt and Lt
paracolic gutters
• right infracolic spaces limited inferiorly by mesentery attachement to IC junction.
• Left Infracolic space connected to pelvis.
17.
PATHALOGIC FINDINGS ANDPATTERNS OF DISEASE SPREAD
• Extraluminal gas
• Fluid collections
• Peritoneal neoplasms
18.
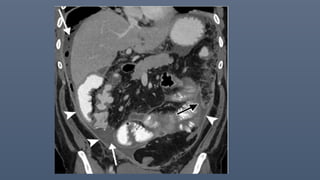
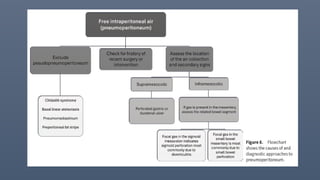
Extraluminal gas (PNEUMOPERITONEUM)
•Free air in peritoneal cavity- sign of bowel perforation
• CT in lung window best – peritoneal recess b/w liver &diaphragm.
• R/O postop/postprocedural causes ( reolved in 3-4D to max 3-4wks).
Others –trauma,recent Sx/intervention,infection by gas producing org
AIR TELLS – SITE OF PERFORATION
2ndry signs – LOCALISED FLUID COLLECTIONS,MESENTRIC FAT STRANDING,FOCAL BOWEL WALL
THICKENING /DEFECT,PNEUMATOSIS
19.
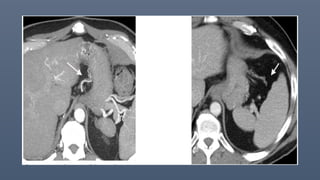
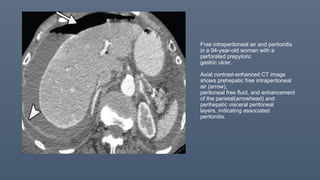
Free intraperitoneal airand peritonitis
in a 94-year-old woman with a
perforated prepyloric
gastric ulcer.
Axial contrast-enhanced CT image
shows prehepatic free intraperitoneal
air (arrow),
peritoneal free fluid, and enhancement
of the parietal(arrowhead) and
perihepatic visceral peritoneal
layers, indicating associated
peritonitis.
21.
FLUID COLLECTIONS
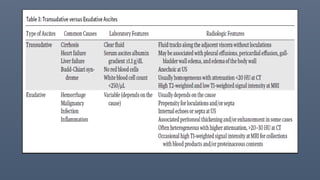
A)Free fluid: transudate vs Exudate
(Infections /Inflamatory /Malignencies)
B)hemorrhage- NCCT - “Sentinel clot “sign ( SOURCE OF BLEEDING )
Hyperattenuating acute clotted blood in close proximity to the source
with lower attenuation non-clotted blood found more distantly
C)Bile – HEPATOBILIARY AGENTS/HIDA SCAN
D)Enteric
E) chylous
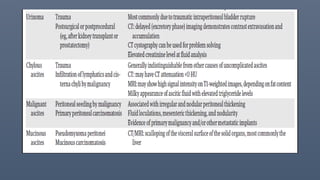
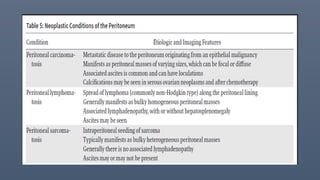
25.
PERITONEAL NEOPLASMS
• Varyingdegrees of peritoneal thickening and soft tissue infiltration,
Mass forming lesions, ascites, calcifications.
Peritoneal metastatic disease is the most common cause of peritoneal
neoplasm
28.
Peritoneal carcinomatosis
• Primary- gastric ,colonic ,appendiceal ,pancreatic ,biliary tract ,and
ovary
• Ascites – early and common feature
• Sheet like growth or infiltration along the mesentry or omentum.
• Thickening and/or enhancement of the peritoneal layers
• Peritoneal implants as suface nodularity /discrete masses
29.
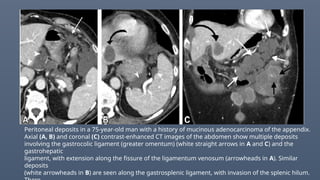
Peritoneal deposits ina 75-year-old man with a history of mucinous adenocarcinoma of the appendix.
Axial (A, B) and coronal (C) contrast-enhanced CT images of the abdomen show multiple deposits
involving the gastrocolic ligament (greater omentum) (white straight arrows in A and C) and the
gastrohepatic
ligament, with extension along the fissure of the ligamentum venosum (arrowheads in A). Similar
deposits
(white arrowheads in B) are seen along the gastrosplenic ligament, with invasion of the splenic hilum.
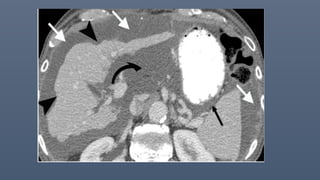
30.
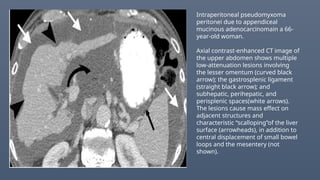
Intraperitoneal pseudomyxoma
peritonei dueto appendiceal
mucinous adenocarcinomain a 66-
year-old woman.
Axial contrast-enhanced CT image of
the upper abdomen shows multiple
low-attenuation lesions involving
the lesser omentum (curved black
arrow); the gastrosplenic ligament
(straight black arrow); and
subhepatic, perihepatic, and
perisplenic spaces(white arrows).
The lesions cause mass effect on
adjacent structures and
characteristic “scalloping”of the liver
surface (arrowheads), in addition to
central displacement of small bowel
loops and the mesentery (not
shown).
31.
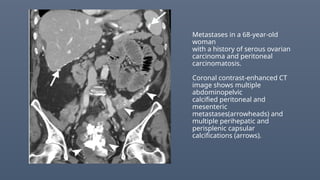
Metastases in a68-year-old
woman
with a history of serous ovarian
carcinoma and peritoneal
carcinomatosis.
Coronal contrast-enhanced CT
image shows multiple
abdominopelvic
calcified peritoneal and
mesenteric
metastases(arrowheads) and
multiple perihepatic and
perisplenic capsular
calcifications (arrows).
32.
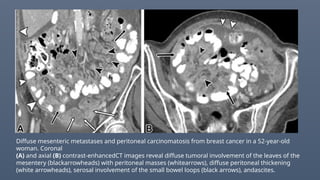
Diffuse mesenteric metastasesand peritoneal carcinomatosis from breast cancer in a 52-year-old
woman. Coronal
(A) and axial (B) contrast-enhancedCT images reveal diffuse tumoral involvement of the leaves of the
mesentery (blackarrowheads) with peritoneal masses (whitearrows), diffuse peritoneal thickening
(white arrowheads), serosal involvement of the small bowel loops (black arrows), andascites.
34.
MIMICS
TB PERITONITIS –smooth uniform thickening of peritoneum
IC junction involvement with necrtotic mesenteric/retroperitoneal
lymphadenopathy with Ancillary findings : granulomas in
liver/spleen/pulmo/mediastinal
35.
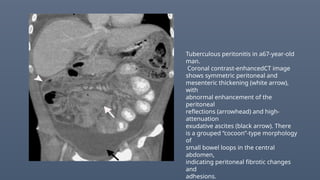
Tuberculous peritonitis ina67-year-old
man.
Coronal contrast-enhancedCT image
shows symmetric peritoneal and
mesenteric thickening (white arrow),
with
abnormal enhancement of the
peritoneal
reflections (arrowhead) and high-
attenuation
exudative ascites (black arrow). There
is a grouped “cocoon”-type morphology
of
small bowel loops in the central
abdomen,
indicating peritoneal fibrotic changes
and
adhesions.
36.
• Peritoneal splenosis-well defined masses mimicking peritoneal
metastasis confirm with MRI USPIO(ferumoxytol) or TC99mm
RBC,TC99mm sulphur colloid scan.
• Encapsulating peritoneal sclerosis (abdominal cacoon )
long term peritoneal dialysis
TB infections
Intraabdominal surgeries
Intraabdominal schunts
Malignencies-Ovarian
37.
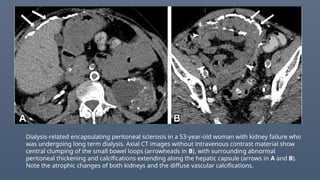
Dialysis-related encapsulating peritonealsclerosis in a 53-year-old woman with kidney failure who
was undergoing long term dialysis. Axial CT images without intravenous contrast material show
central clumping of the small bowel loops (arrowheads in B), with surrounding abnormal
peritoneal thickening and calcifications extending along the hepatic capsule (arrows in A and B).
Note the atrophic changes of both kidneys and the diffuse vascular calcifications.
38.
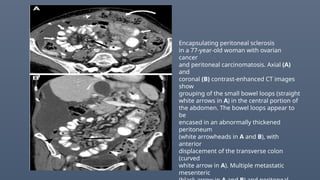
Encapsulating peritoneal sclerosis
ina 77-year-old woman with ovarian
cancer
and peritoneal carcinomatosis. Axial (A)
and
coronal (B) contrast-enhanced CT images
show
grouping of the small bowel loops (straight
white arrows in A) in the central portion of
the abdomen. The bowel loops appear to
be
encased in an abnormally thickened
peritoneum
(white arrowheads in A and B), with
anterior
displacement of the transverse colon
(curved
white arrow in A). Multiple metastatic
mesenteric
39.
• Calcified peritonealdeposits in absence of chemotheraphy
serous ovarian neoplasm or mucinous neoplasms of
gastric/colon/appendix.
40.
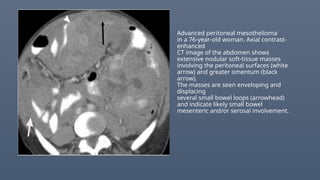
Advanced peritoneal mesothelioma
ina 76-year-old woman. Axial contrast-
enhanced
CT image of the abdomen shows
extensive nodular soft-tissue masses
involving the peritoneal surfaces (white
arrow) and greater omentum (black
arrow).
The masses are seen enveloping and
displacing
several small bowel loops (arrowhead)
and indicate likely small bowel
mesenteric and/or serosal involvement.
41.
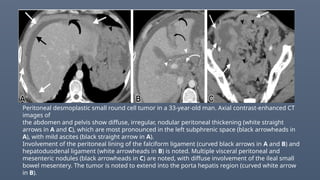
Peritoneal desmoplastic smallround cell tumor in a 33-year-old man. Axial contrast-enhanced CT
images of
the abdomen and pelvis show diffuse, irregular, nodular peritoneal thickening (white straight
arrows in A and C), which are most pronounced in the left subphrenic space (black arrowheads in
A), with mild ascites (black straight arrow in A).
Involvement of the peritoneal lining of the falciform ligament (curved black arrows in A and B) and
hepatoduodenal ligament (white arrowheads in B) is noted. Multiple visceral peritoneal and
mesenteric nodules (black arrowheads in C) are noted, with diffuse involvement of the ileal small
bowel mesentery. The tumor is noted to extend into the porta hepatis region (curved white arrow
in B).
42.
Pathways of neoplasticperitoneal disease spread
• Peritoneal carcinomatosis – sites of fluid stasis or reabsorption.
• Direct invasion
• Hematogeneous
• Lymphatics –NHL, gastric and ovarian
• Kruken berg tumours – bilateral mixed solid and cystic ovarian masses
where primary malignancy from GIT.
Transperitoneal/hematogeneous/retrograde lymphatics
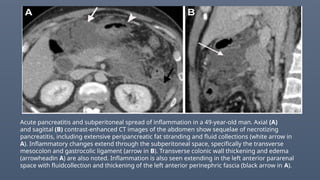
Acute pancreatitis andsubperitoneal spread of inflammation in a 49-year-old man. Axial (A)
and sagittal (B) contrast-enhanced CT images of the abdomen show sequelae of necrotizing
pancreatitis, including extensive peripancreatic fat stranding and fluid collections (white arrow in
A). Inflammatory changes extend through the subperitoneal space, specifically the transverse
mesocolon and gastrocolic ligament (arrow in B). Transverse colonic wall thickening and edema
(arrowheadin A) are also noted. Inflammation is also seen extending in the left anterior pararenal
space with fluidcollection and thickening of the left anterior perinephric fascia (black arrow in A).
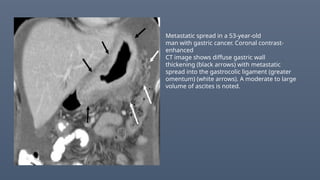
Metastatic spread ina 53-year-old
man with gastric cancer. Coronal contrast-
enhanced
CT image shows diffuse gastric wall
thickening (black arrows) with metastatic
spread into the gastrocolic ligament (greater
omentum) (white arrows). A moderate to large
volume of ascites is noted.
50.
• NETs –mesntrialmets as Aretrial enhancing mass with calcifications
and desmoplastic reaction – tethering of adjascent bowel loops
• Desmoid tumours of mesentry Locally invasive fibroblastic tumours
(association FAP)
• Mesentric panniculitis : can be associated with IGG4D
Acute – Fat Halo sign
Chronic – mass formation with desmoplastic reaction/calcifications
51.
• Ascending anddescending Mesocolon- colonic ca
• Direct invasion - Loss of fat plane b/w tumour and mesocolon , soft
tissue thickening or masses in the mesocolon and irregularity and
distortions of adjascent structures.
• Regional LN
• Paracolic and intermediate mesocolic LN---- root of mesntric LN along
SMA/IMA
52.
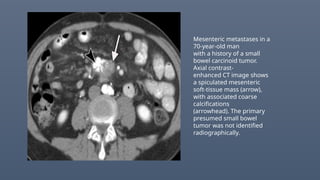
Mesenteric metastases ina
70-year-old man
with a history of a small
bowel carcinoid tumor.
Axial contrast-
enhanced CT image shows
a spiculated mesenteric
soft-tissue mass (arrow),
with associated coarse
calcifications
(arrowhead). The primary
presumed small bowel
tumor was not identified
radiographically.
53.
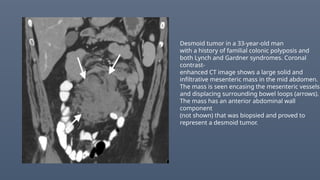
Desmoid tumor ina 33-year-old man
with a history of familial colonic polyposis and
both Lynch and Gardner syndromes. Coronal
contrast-
enhanced CT image shows a large solid and
infiltrative mesenteric mass in the mid abdomen.
The mass is seen encasing the mesenteric vessels
and displacing surrounding bowel loops (arrows).
The mass has an anterior abdominal wall
component
(not shown) that was biopsied and proved to
represent a desmoid tumor.
54.
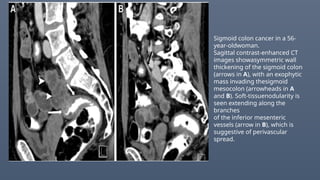
Sigmoid colon cancerin a 56-
year-oldwoman.
Sagittal contrast-enhanced CT
images showasymmetric wall
thickening of the sigmoid colon
(arrows in A), with an exophytic
mass invading thesigmoid
mesocolon (arrowheads in A
and B). Soft-tissuenodularity is
seen extending along the
branches
of the inferior mesenteric
vessels (arrow in B), which is
suggestive of perivascular
spread.
55.
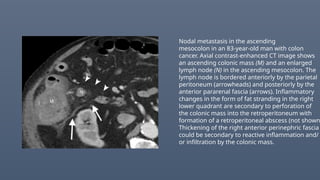
Nodal metastasis inthe ascending
mesocolon in an 83-year-old man with colon
cancer. Axial contrast-enhanced CT image shows
an ascending colonic mass (M) and an enlarged
lymph node (N) in the ascending mesocolon. The
lymph node is bordered anteriorly by the parietal
peritoneum (arrowheads) and posteriorly by the
anterior pararenal fascia (arrows). Inflammatory
changes in the form of fat stranding in the right
lower quadrant are secondary to perforation of
the colonic mass into the retroperitoneum with
formation of a retroperitoneal abscess (not shown
Thickening of the right anterior perinephric fascia
could be secondary to reactive inflammation and/
or infiltration by the colonic mass.
56.
PERINEURAL SPREAD
• Ifnerve visible -Nodular thickening
• if nerve not visible – Abnormal soft tissue thickening extending along
the blood vessels adjacent to primary tumour
• Eg : pancreatic malignancy along the SMA
Colorectal,prostatic ,cervical,gastric ,biliary malignencies, lymphoma
Poor prognosis
High risk of recurrance
57.
Lymphatic spread
Pancreatic head& UP –along SMA ,root of mesentry
Pancreatic body & Tail – along celiac,hepatic and splenic A
Bowel maligencies : Bowel wall thickening and edema
Thickened mucosal folds
Loss of colonic haustrations
Stranding of surrounding mesenteric fat
Poor prognosis.
58.
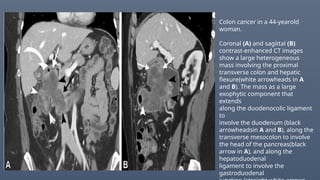
Colon cancer ina 44-yearold
woman.
Coronal (A) and sagittal (B)
contrast-enhanced CT images
show a large heterogeneous
mass involving the proximal
transverse colon and hepatic
flexure(white arrowheads in A
and B). The mass as a large
exophytic component that
extends
along the duodenocolic ligament
to
involve the duodenum (black
arrowheadsin A and B), along the
transverse mesocolon to involve
the head of the pancreas(black
arrow in A), and along the
hepatoduodenal
ligament to involve the
gastroduodenal
59.
CONCLUSION
• The anatomyof the peritoneum, subperitoneum, and related ligaments and
spaces is complex.
• The peritoneal cavity and its fluid flow dynamics, membranes, peritoneal
ligaments,and subperitoneal spaces form potential spaces and pathways
for the spread of a myriad of neoplastic and nonneoplastic abnormalities.
• Understanding the embryology, anatomy, and various classifications of the
peritoneum is crucial for recognizing and accurately describing patterns of
disease spread in the peritoneum.









































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)










