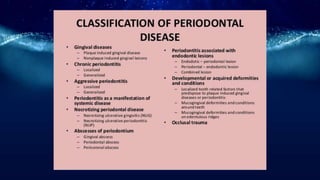
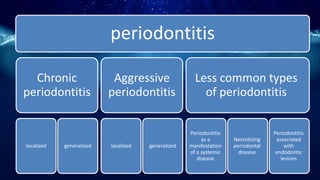
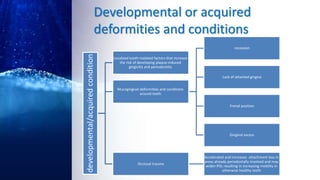
This document summarizes different types of periodontal diseases including gingivitis, chronic periodontitis, aggressive periodontitis, necrotizing periodontal disease, periodontitis associated with systemic diseases, and abscesses of the periodontium. It describes the clinical features, risk factors, stages of progression, and treatment for each type of periodontal disease. Developmental deformities and conditions are also outlined that can increase the risk of plaque-induced gingivitis and periodontitis.

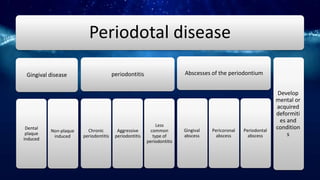
















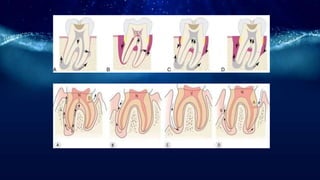

![Abscesses of the periodontium
• Gingival abscess—a localized, purulent infection
involves only the soft gum tissue near the marginal
gingiva or the interdental papilla.[3]
• Periodontal abscess—a localized, purulent infection
involving a greater dimension of the gum tissue,
extending apically and adjacent to a periodontal
pocket.[3]
• Pericoronal abscess—a localized, purulent infection
within the gum tissue surrounding the crown of a
partially or fully erupted tooth.[3] Usually associated
with an acute episode of pericoronitis around a
partially erupted and impacted mandibular third
molar (lower wisdom tooth).](https://image.slidesharecdn.com/periodontaldiseaseautosaved-180619020747/85/Periodontal-disease-autosaved-39-320.jpg)

![Periodontal disease [autosaved]](https://image.slidesharecdn.com/periodontaldiseaseautosaved-180619020747/85/Periodontal-disease-autosaved-42-320.jpg)

































































