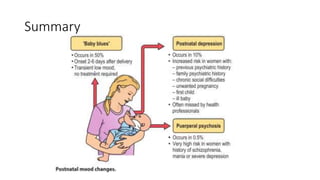
This document discusses various postpartum psychiatric disorders including postpartum blues, postpartum depression, and postpartum psychosis. Postpartum blues occurs in 50% of women within 2-6 days of delivery and involves transient low mood but is typically self-limiting within a few days. Postpartum depression occurs in 10% of women within the first 6 weeks and can involve feelings of guilt, anxiety about the baby, and reluctance to care for the baby. Risk factors include a history of depression and relationship or baby related stressors. Postpartum psychosis occurs in 0.5% of women and involves an abrupt onset of affective or manic symptoms within 2-4 weeks of delivery that usually requires






![Post Partum Disorders [2001]](https://cdn.slidesharecdn.com/ss_thumbnails/postpartum-170814005829-thumbnail.jpg?width=640&height=640&fit=bounds)










![Non-delusional Morbid Jealousy [2019]](https://cdn.slidesharecdn.com/ss_thumbnails/56201795113132228753-190801100249-thumbnail.jpg?width=640&height=640&fit=bounds)




































































