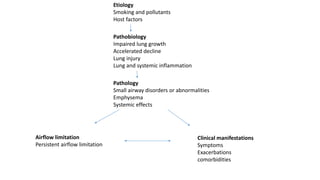
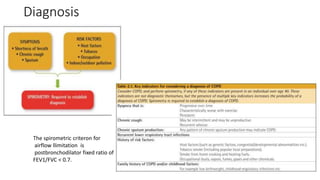
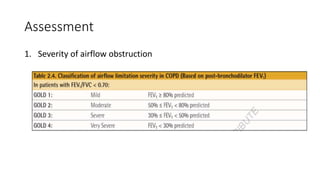
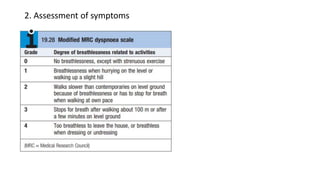
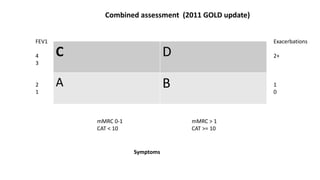
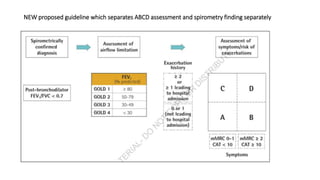
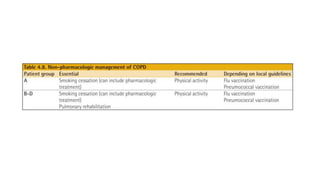
This document summarizes the revised GOLD guidelines for assessing COPD. It defines COPD as a preventable disease characterized by airflow limitation caused by exposure to particles or gases. The assessment includes evaluating the severity of airflow obstruction, symptoms, exacerbation risk, and comorbidities. The revised guidelines separate the ABCD assessment based on symptoms and exacerbation history from spirometric findings, allowing treatment to be initiated based on symptoms alone when spirometry is unavailable.



![PT management in CKD [Renal Rehabilitation].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ptmanagementinckdrenalrehabilitation-220727071020-ee721238-thumbnail.jpg?width=640&height=640&fit=bounds)


















































































